

-
摘要:
目的 探讨肝移植供肝合并局灶性结节增生(FNH)及肝右动脉变异的处理方法。 方法 2013年11月实施1例供肝存在FNH合并肝右动脉变异的经典原位肝移植术。供肝修整过程中切除肝脏占位病变,快速冰冻病理检查证实为FNH,并将变异肝右动脉的肠系膜上动脉补片与脾动脉端端吻合。 结果 供肝变异动脉修整重建后成功完成供肝植入,术后无动脉血栓形成、胆漏、出血等相关并发症。 结论 当供肝肝右动脉起源于肠系膜上动脉时,首选变异肝右动脉的肠系膜上动脉补片与脾动脉端端吻合。供肝FNH并非肝移植的禁忌证,可在修肝过程中予以一期切除。 -

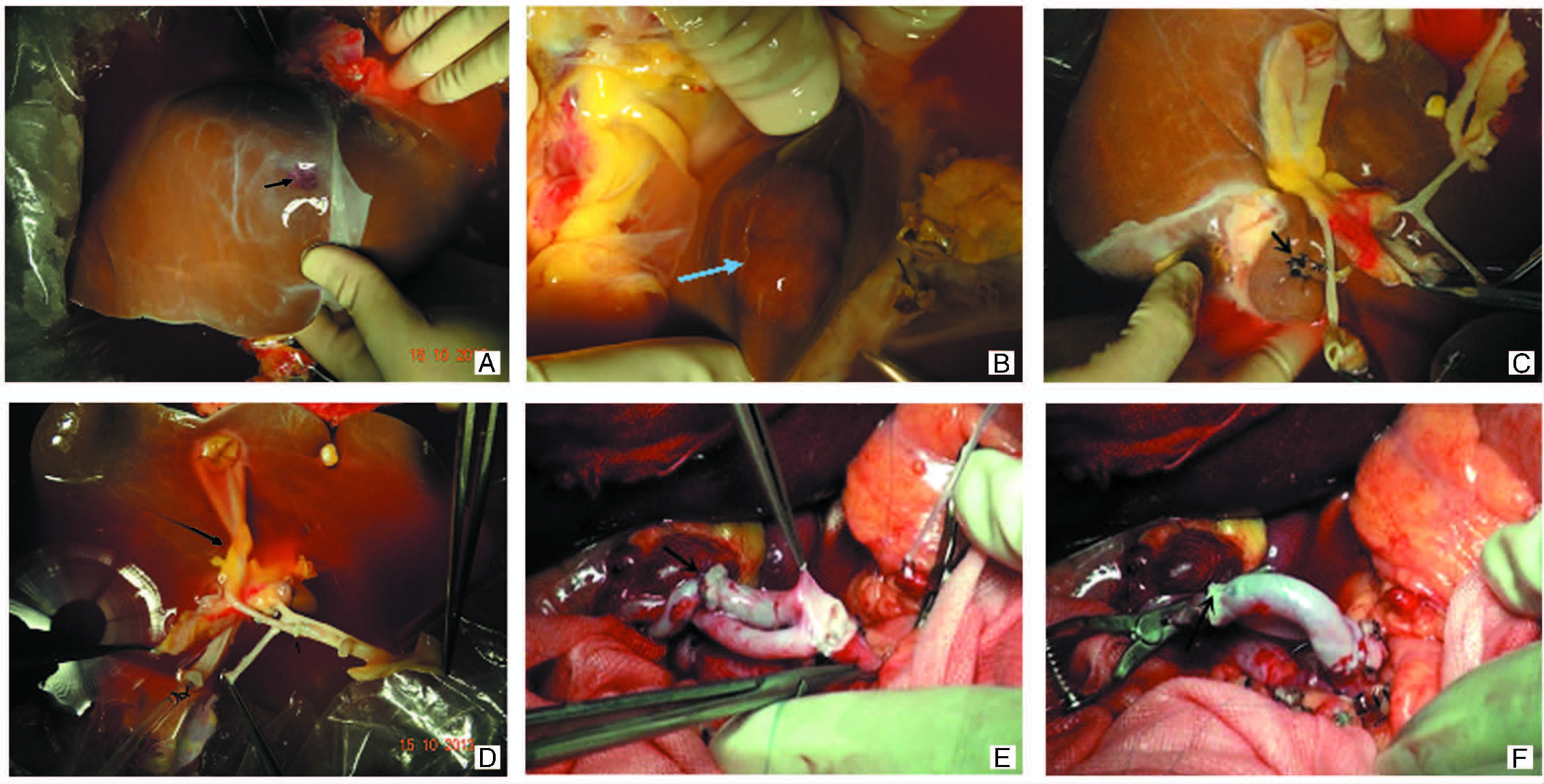
图 1 本例受者的手术过程图
注:A图于供肝左内叶见大小约1.5 cm血管瘤(黑色箭头所示);B图为尾叶肿瘤(蓝色箭头所示);C图为尾叶肿瘤切除后(黑色箭头所示);D图示变异肝右动脉的肠系膜上动脉补片与脾动脉吻合口(黑色箭头所示);E图示供受者动脉吻合,箭头所示变异肝右动脉的补片与脾动脉吻合口;F图示肝动脉重建后复流,箭头所示变异肝右动脉的补片与脾动脉吻合口
Figure 1. The photograph of operation procedure of the recipient

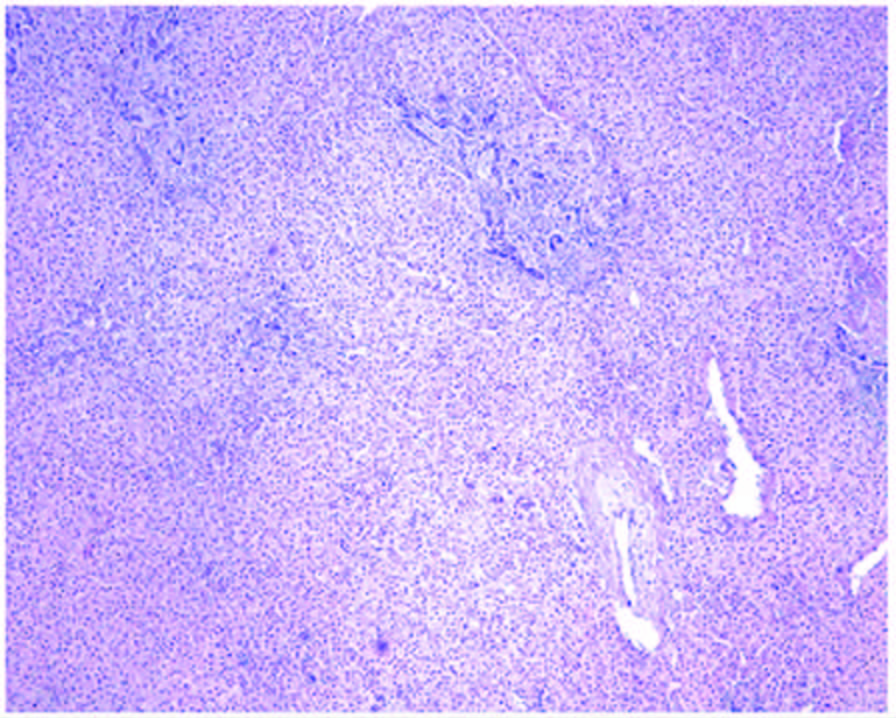
图 2 尾叶肿瘤快速冰冻病理示肝脏局灶性 结节样增生(苏木素-伊红,×100)
Figure 2. Intraoperative frozen pathology indicated that caudate lobe neoplasm was the focal nodular hyperplasia

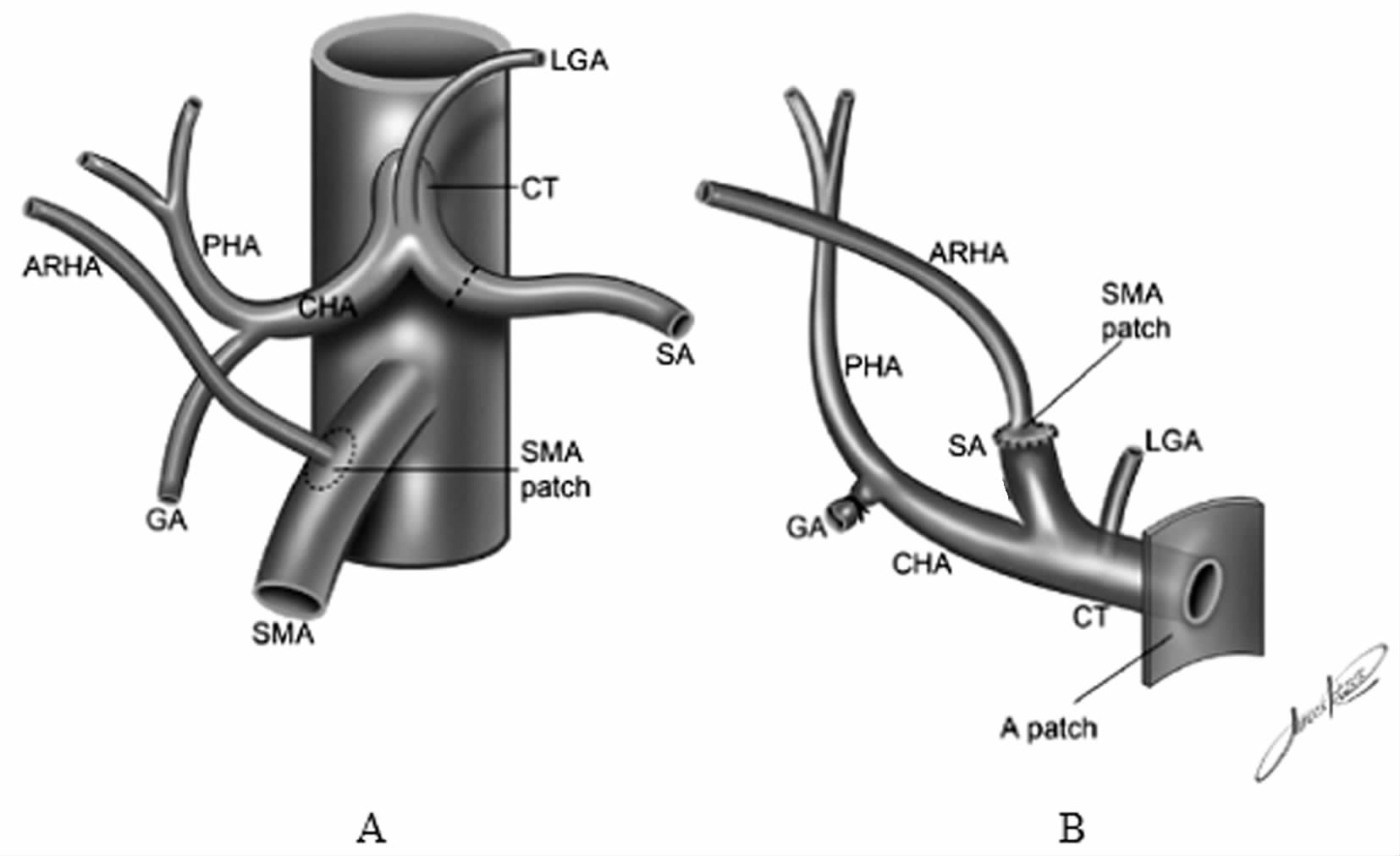
图 3 供肝变异血管处理示意图
注:ARHA为变异的肝右动脉,GA为胃十二指肠动脉,SMA为肠系膜上动脉,PHA为肝固有动脉,CHA为肝总动脉,SA为脾动脉,CT为腹腔干,LGA为胃左动脉,patch为补片[本图引自Andraus W,Haddad LB,Ducatti L,et al. Artery reconstruction in liver transplantation: the best reconstruction of right hepatic artery variation[J]. Arq Bras Cir Dig(葡萄牙文),2013,26(1):62-65.]
Figure 3. Schematic diagram of management of variant blood vessel in donor liver
表 1 本例接受肝脏局灶性结节增生供肝受者术后肝功能变化情况
Table 1. Postoperative liver function of the liver transplant recipient with focal nodular hyperplasia
术后时间(d) ALT(U/L) AST(U/L) ALP(U/L) Alb(g/L) TB(μmol/L) DB(μmol/L) 2 299 137 53 34 18.9 9.3 3 192 47 47 39 9.7 5.2 4 128 29 47 38 11.4 5.1 6 76 20 51 41 22.5 8.9 7 112 42 70 36 24.2 13 8 153 48 80 32 29.8 18.6 9 151 46 142 31 24.3 15.8 10 140 39 111 30 14.3 9.1 11 102 23 104 30 12.9 7.7 13 59 18 101 36 18.7 8.8 14 44 19 91 38 17.9 8.4 16 40 30 82 36 17.7 8.4 17 46 37 82 36 14.1 6.6 18 45 31 75 35 14.8 6.6 注:ALT为丙氨酸转氨酶,AST为天冬氨酸转氨酶,ALP为碱性磷酸酶(alkaline phosphatase),Alb为白蛋白(albumin),TB为总胆红素(total bilirubin),DB为直接胆红素(direct bilirubin)  下载: 导出CSV
下载: 导出CSV
-
[1] Choi JY, Lee HC, Yim JH, et al. Focal nodular hyperplasia or focal nodular hyperplasia-like lesions of the liver: a special emphasis on diagnosis[J]. J Gastroenterol Hepatol, 2011, 26(6):1004-1009. doi: 10.1111/j.1440-1746.2011.06659.x [2] Ungermann L, Eliás P, Zizka J, et al. Focal nodular hyperplasia: spoke-wheel arterial pattern and other signs on dynamic contrast-enhanced ultrasonography[J]. Eur J Radiol,2007,63(2):290-294. doi: 10.1016/j.ejrad.2007.01.026 [3] 赵红川,耿小平. 无心跳供体肝肾等器官快速切取技术[J]. 肝胆外科杂志,2010,18(3):228-229. http://www.cnki.com.cn/Article/CJFDTOTAL-GDWZ201003031.htmZhao HC,Geng XP. Technique of rapid procurement of liver,kidney and so on from cardiac death donor[J]. J Hepatobiliary Surg, 2010,18(3):228-229. http://www.cnki.com.cn/Article/CJFDTOTAL-GDWZ201003031.htm [4] Andraus W, Haddad LB, Ducatti L, et al. Artery reconstruction in liver transplantation: the best reconstruction of right hepatic artery variation[J]. Arq Bras Cir Dig(葡萄牙文),2013, 26(1):62-65. doi: 10.1590/S0102-67202013000100014 [5] Hiatt JR, Gabbay J, Busuttil RW.Surgical anatomy of the hepatic arteries in 1000 cases[J]. Ann Surg,1994,220(1):50-52. doi: 10.1097/00000658-199407000-00008 [6] 杨扬,姜楠,陆敏强,等. 843例肝移植供肝动脉的解剖变异分析[J].南方医科大学学报,2007,27(8):1164-1166. http://www.cnki.com.cn/Article/CJFDTOTAL-DYJD200708012.htmYang Y, Jiang N, Lu MQ,et al. Anatomical variation of the donor hepatic arteries: analysis of 843 cases[J].Nan Fang Yi Ke Da Xue Xue Bao, 2007, 27(8):1164-1166. http://www.cnki.com.cn/Article/CJFDTOTAL-DYJD200708012.htm [7] Nat L, Poant LI.Focal nodular hyperplasia(FNH).Rom J Intern Med,2014,52(1):45-49. http://cn.bing.com/academic/profile?id=2102743402&encoded=0&v=paper_preview&mkt=zh-cn [8] Melin C, Miick R, Young NA, et al. Approach to intraoperative consultation for donor liver biopsies[J]. Arch Pathol Lab Med, 2013, 137(2):270-274. doi: 10.5858/arpa.2011-0689-RA [9] Tan M, Di Carlo A, Robinson P, et al. Successful outcome after transplantation of a donor liver with focal nodular hyperplasia[J]. Liver Transpl,2001,7(7):652-655. doi: 10.1053/jlts.2001.23910 [10] Bieze M, Phoa SS, Verheij J, et al. Risk factors for bleeding in hepatocellular adenoma[J]. Br J Surg, 2014,101(7):847-855. doi: 10.1002/bjs.2014.101.issue-7 -

 下载:
下载:

 点击查看大图
点击查看大图
计量
- 文章访问数: 143
- HTML全文浏览量: 128
- PDF下载量: 4
- 被引次数: 0


