Abstract:
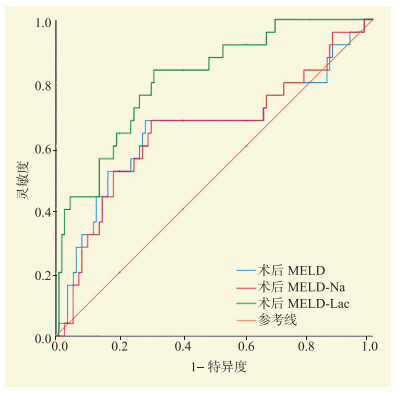
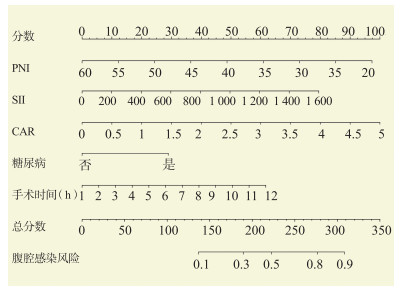
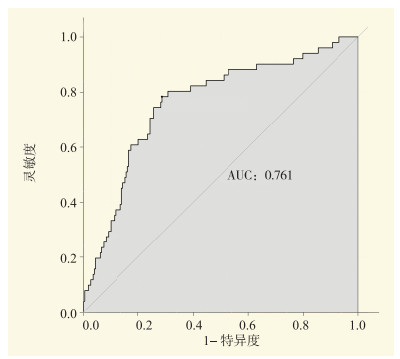
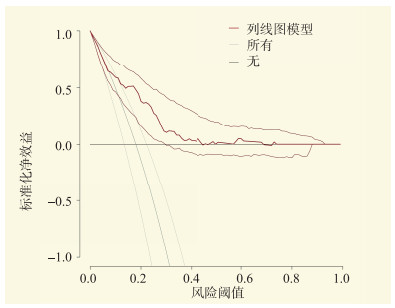
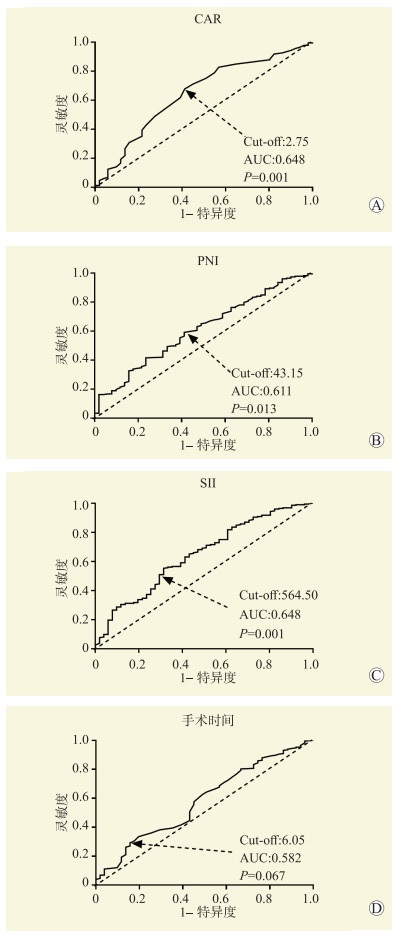
Objective To investigate the risk factors of abdominal infection after orthotopic liver transplantation. Methods Clinical data of 284 recipients undergoing orthotopic liver transplantation were retrospectively analyzed. All recipients were divided into the infection group (n=51) and non-infection group (n=233) according to the incidence of postoperative abdominal infection. Univariate and multivariate logistic regression analyses were used to identify the risk factors of abdominal infection. Nomogram prediction models were constructed and the prediction efficiency of these models was evaluated. The predictive value of continuous variables for abdominal infection was assessed. Results Among 284 recipients, 51 developed abdominal infection with an incidence of 18.0%. Diabetes mellitus before surgery[odds ratio (OR) 2.66, 95% confidence interval (CI) 1.13-6.14, P=0.013], long operation time (OR 1.98, 95%CI 1.03-3.57, P=0.038), low prognostic nutritional index (PNI) (OR 2.18, 95%CI 1.06-4.44, P=0.023), high systemic immune-inflammation index (SII) (OR 2.21, 95%CI 1.06-4.78, P=0.012) and high C-reactive protein/albumin ratio (CAR) (OR 1.90, 95%CI 1.05-3.49, P=0.029) were independent risk factors for abdominal infection after liver transplantation. The area under curve (AUC) of nomogram model for predicting abdominal infection after liver transplantation was 0.761. The standard model yielded high consistency. CAR, PNI and SII were all predictors of abdominal infection after liver transplantation (all P < 0.05), with AUC of 0.648, 0.611 and 0.648, and cut-off values of 2.75, 43.15 and 564.50, respectively. Conclusions CAR, SII and PNI are predictors of abdominal infection after liver transplantation. The nomogram model based on PNI, SII and CAR may effectively predict the incidence of abdominal infection after liver transplantation.