

Distribution characteristics of pathogenic bacteria in infectious donors from organ donation after citizen's death and preventive strategies for renal transplant recipients: a single center experience
-
摘要:
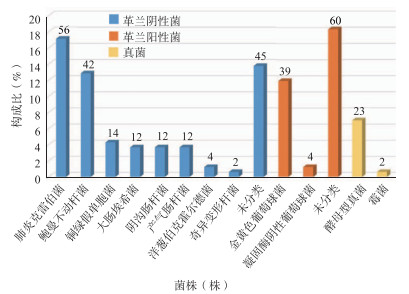
目的 探讨公民逝世后器官捐献供者感染病原菌分布特点及肾移植受者预防策略。 方法 回顾性分析412例公民逝世后器官捐献供者及对应803例受者临床资料,所有供者均行气道分泌物、尿液、血液及供肾灌洗液培养,观察公民逝世后器官捐献供者感染发生率、病原菌分布和构成比,根据供者重症监护室(ICU)住院时间、腹部外伤情况、体液培养结果等因素进行评分,受者根据评分采用不同的感染预防方案,分析供者来源性感染(DDI)的发生率及受者预后。 结果 412例公民逝世后器官捐献供者中共有243例存在感染,感染率59.0%,共分离出病原菌456株,病原菌主要来源于气道分泌物(71.7%)。革兰阴性菌以肺炎克雷伯菌和鲍曼不动杆菌为主,革兰阳性菌以金黄色葡萄球菌为主,真菌主要为酵母型真菌。共有3例受者(分别接受来自2例供者的肾脏)发生DDI,发生率0.4%。 结论 公民逝世后器官捐献供者感染率较高,对供者感染风险进行分级评分,根据评分采取合理预防方案,可有效预防DDI。 Abstract:Objective To investigate the distribution characteristics of pathogenic bacteria in infectious donors from organ donation after citizen's death and preventive strategies for renal transplant recipients. Methods Clinical data of 412 donors and 803 recipients from organ donation after citizen's death were retrospectively analyzed. All donors underwent culture of airway secretions, urine, blood and renal lavage fluid. The incidence rate of infection, distribution and composition ratio of pathogenic bacteria of donors from organ donation after citizen's death were observed. The scores of all donors were evaluated according to the length of intensive care unit (ICU) stay for donors, the situation of abdominal trauma and the results of body fluid culture, etc. According to the score, the recipients received different infection prevention regimes. The incidence rate of donor-derived infection (DDI) and clinical prognosis of the recipients were analyzed. Results A total of 243 donors were diagnosed with infection in 412 donors from organ donation after citizen's death with an infection rate of 59.0%. In total, 456 strains of pathogenic bacteria were isolated, mainly derived from the airway secretions (71.7%). Gram-negative bacteria dominantly consisted of Klebsiella pneumoniae and acinetobacter baumannii. Gram-positive bacteria mainly included staphylococcus aureus and fungus mainly included yeast-type fungus. Three recipients (kidneys from 2 donors respectively) developed DDI with an incidence rate of 0.4%. Conclusions The infection rate of donors from organ donation after citizen's death is relatively high. It is effective to prevent the incidence of DDI by grading the risk of infection of donors and adopting rational preventive plan according to the score. -

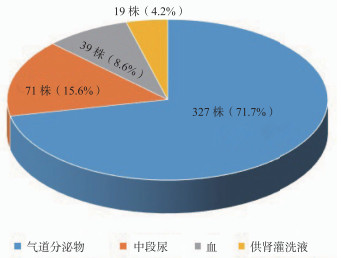
图 1 供者感染病原菌来源分布
Figure 1. Source distribution of pathogenicbacteria in infected donors

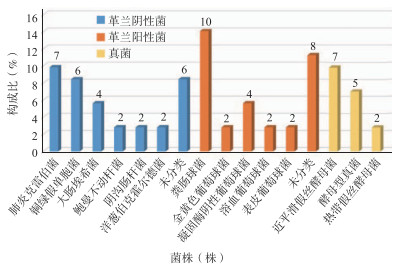
图 2 供者气道分泌物培养阳性菌株分布
Figure 2. Distribution of positive bacteria strains cultured in airway secretions of donors

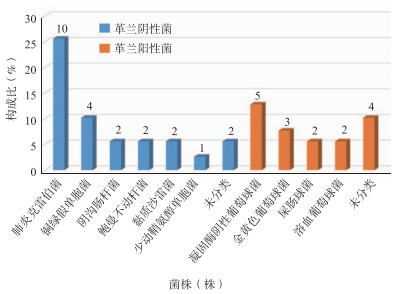
图 3 供者中段尿培养阳性菌株分布
Figure 3. Distribution of positive bacteria strains cultured in midstream urine of donors

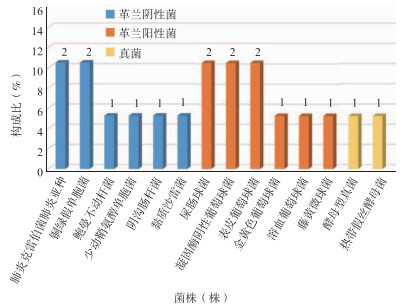
图 4 供者血培养阳性菌株分布
Figure 4. Distribution of positive bacteria strains cultured in blood of donors

图 5 供肾灌洗液培养阳性菌株分布
Figure 5. Distribution of positive bacteria strains cultured in donor kidney lavage solution
表 1 供者感染风险评分标准
Table 1. Scoring criteria of donor infection risk
分类 评分 ICU住院时间(d) < 3 0 3~7 1 > 7 2 腹部外伤情况 无腹部外伤 0 腹部闭合性损伤 1 腹部开放性损伤 2 体液培养情况 体液培养(-) 0 痰培养(+) 1 中段尿培养(+) 2 供肾灌洗液/血培养(+) 3  下载: 导出CSV
下载: 导出CSV
表 2 供者来源性感染受者病原菌分布情况
Table 2. Distribution of pathogenic bacteria from recipients with donor-derived infection
例序 性别 年龄
(岁)预防方案 痰培养 中段尿 血培养 肾周引流液 住院时间(d) 受者1 男 48 三联预防 铜绿假单胞菌 - CRE(+)和ESBL(+)肺炎克雷伯菌 CRE(+)肺炎克雷伯菌 29 受者2 女 30 三联预防 - - CRE(+)和ESBL(+)肺炎克雷伯菌 CRE(+)肺炎克雷伯菌 82 受者3 男 42 三联预防 - - - - 14 受者4 男 34 三联预防 铜绿假单胞菌 热带假丝酵母菌 - - 20 受者1、2的供肾均来自供者1,受者3、4的供肾均来自供者2
下载: 导出CSV
-
[1] ZHANG L, ZENG L, GAO X, et al. Transformation of organ donation in China[J]. Transpl Int, 2015, 28(4):410-415. DOI: 10.1111/tri.12467. [2] DOUCETTE KE, AL-SAIF M, KNETEMAN N, et al. Donor-derived bacteremia in liver transplant recipients despite antibiotic prophylaxis[J]. Am J Transplant, 2013, 13(4):1080-1083. DOI: 10.1111/ajt.12133. [3] CAMARGO JF. Donor-derived infections in solid organ transplant recipients: challenging the 30-day paradigm[J]. Transpl Infect Dis, 2017, 19(2). DOI: 10.1111/tid.12665. [4] BEGAJ I, KHOSLA S, RAY D, et al. Socioeconomic deprivation is independently associated with mortality post kidney transplantation[J]. Kidney Int, 2013, 84(4):803-809. DOI: 10.1038/ki.2013.176. [5] GROSSI PA, COSTA AN, FEHILY D, et al. Infectionsand organ transplantation: new challenges for preventionand treatment--a colloquium[J]. Transplantation, 2012, 93 (5 Suppl):S4-S39. DOI: 10.1097/TP.0b013e3182481347. [6] 尚红, 王毓三, 申子瑜.全国临床检验操作规程[M]. 4版.北京:人民卫生出版社, 2015:629-638. [7] AVERY RK, LJUNGMAN P. Prophylactic measures in the solid-organ recipient before transplantation[J].Clin Infect Dis, 2001, 33 (Suppl 1):S15-S21. DOI:10.1086/ 320899. [8] FISHMAN JA, ISSA NC. Infection in organ transplantation: risk factors and evolving patterns of infection[J]. Infect Dis Clin North Am, 2010, 24(2):273-283. DOI: 10.1016/j.idc.2010.01.005. [9] ISON MG, GROSSI P, AST Infectious Diseases Community of Practice. Donor-derived infections in solid organ transplantation[J]. Am J Transplant, 2013, 13 (Suppl 4):22-30. DOI: 10.1111/ajt.12095. [10] SINGH N. Impact of donor bacteremia on outcomein organ transplant recipients[J]. Liver Transpl, 2002, 8(10):975-976. DOI: 10.1053/jlts.2002.0080975. [11] LEWIS JD, SIFRI CD. Multidrug-resistant bacterialdonor-derived infections in solid organ transplantation[J]. Curr Infect Dis Rep, 2016, 18(6):18. DOI: 10.1007/s11908- 016-0526-9. [12] 中华医学会器官移植学分会.器官移植供者来源性感染诊疗技术规范(2019版)[J].器官移植, 2019, 10(4):369-375. DOI: 10.3969/j.issn.1674-7445.2019.04.005.Branch of Organ Transplantation of Chinese Medical Association. Technical specification for diagnosis and treatment of donor-derived infection in organ transplantation (2019 edition)[J]. Organ Transplant, 2019, 10(4):369-375. DOI: 10.3969/j.issn.1674-7445.2019.04.005. [13] BENAMU E, WOLFE CR, MONTOYA JG. Donor-derived infections in solid organ transplant patients: toward a holistic approach[J]. Curr Opin Infect Dis, 2017, 30(4):329-339. DOI: 10.1097/QCO.0000000000000377. [14] WAN Q, LIU H, YE S, et al. Confirmed transmission of bacterial or fungal infection to kidney transplant recipients from donated after cardiac death (DCD) donors in China: a single-center analysis[J]. Med Sci Monit, 2017, 23:3770-3779. DOI: 10.12659/msm.901884. [15] 何莉, 林栋栋, 刘晋宁, 等.公民器官捐献供者感染现状与应对的回顾性研究[J].北京医学, 2019, 41(6):472-475. DOI: 10.15932/j.0253-9713.2019.06.009.HE L, LIN DD, LIU JN, et al. A retrospective study on the current situation and coping strategies of organ donor infection[J]. Beijing Med J, 2019, 41(6):472-475. DOI: 10.15932/j.0253-9713.2019.06.009. [16] 汪海源, 洪涛, 吴兴茂, 等. ICU内获得性感染细菌谱的时间分布分析[J].中国医科大学学报, 2015, 44(5):434-437. DOI: 10.3969/j.issn.0258-4646.2015.05.011.WANG HY, HONG T, WU XM, et al. Analysis of bacterial time distribution of ICU-acquired infections[J]. J Chin Med Univ, 2015, 44(5):434-437. DOI: 10.3969/j.issn.0258-4646.2015.05.011. [17] JOVANOVI M, TOP J, MAJOOR E, et al. Multiplelocus variable number tandem repeat analysis typing of vancomycin-resistant Enterococcus faecium in Serbia[J]. Infect Control Hosp Epidemiol, 2013, 34(12):1337-1339. DOI: 10.1086/673990. [18] BAO L, PENG R, REN X, et al. Analysis of some common pathogens and their drug resistance to antibiotics[J]. Pak J Med Sci, 2013, 29(1):135-139. DOI: 10.12669/pjms. 291.2744. [19] MARTIN-LOECHES I, RODRIGUEZ AH, TORRES A.New guidelines for hospital-acquired pneumonia/ventilator-associated pneumonia: USA vs. Europe[J]. Curr Opin Crit Care, 2018, 24(5):347-352. DOI:10.1097/MCC. 0000000000000535. [20] CHOI WS, KIM SH, JEON EG, et al. Nosocomialoutbreak of carbapenem-resistant acinetobacter baumannii in intensive care units and successful outbreak control program[J]. J Korean Med Sci, 2010, 25(7):999-1004. DOI: 10.3346/jkms.2010.25.7.999. [21] DEN HEIJER CD, VAN BIJNEN EM, PAGET WJ, et al. Prevalence and resistance of commensal Staphylococcus aureus, including meticillin-resistant S aureus, in nine European countries: a cross-sectional study[J]. Lancet Infect Dis, 2013, 13(5):409-415. DOI: 10.1016/S1473-3099(13)70036-7. [22] ESCOLÀ-VERGÉ L, LOS-ARCOS I, JOSÉ GONZÁLEZ-LÓPEZ J, et al. Successful liver transplantation despite donor-transmitted ESBL-producing Klebsiella pneumoniae infection: case report and review of the literature[J]. Transpl Infect Dis, 2017, 19(5). DOI: 10.1111/tid.12743. [23] MILLS JP, WILCK MB, WEIKERT BC, et al. Successful treatment of a disseminated infection with extensively drug-resistant Klebsiella pneumoniae in a liver transplant recipient with a fosfomycin-based multidrug regimen[J]. Transpl Infect Dis, 2016, 18(5):777-781. DOI: 10.1111/tid.12578. [24] GREEN M, COVINGTON S, TARANTO S, et al. Donor-derived transmission events in 2013: a report of the Organ Procurement Transplant Network Ad Hoc Disease Transmission Advisory Committee[J]. Transplantation, 2015, 99(2):282-287. DOI: 10.1097/TP.0000000000000584. -

 下载:
下载:

 点击查看大图
点击查看大图
计量
- 文章访问数: 136
- HTML全文浏览量: 49
- PDF下载量: 29
- 被引次数: 0


