

Comparison of application value of three pulmonary infection scoring systems in pulmonary infection after renal transplantation
-
摘要:
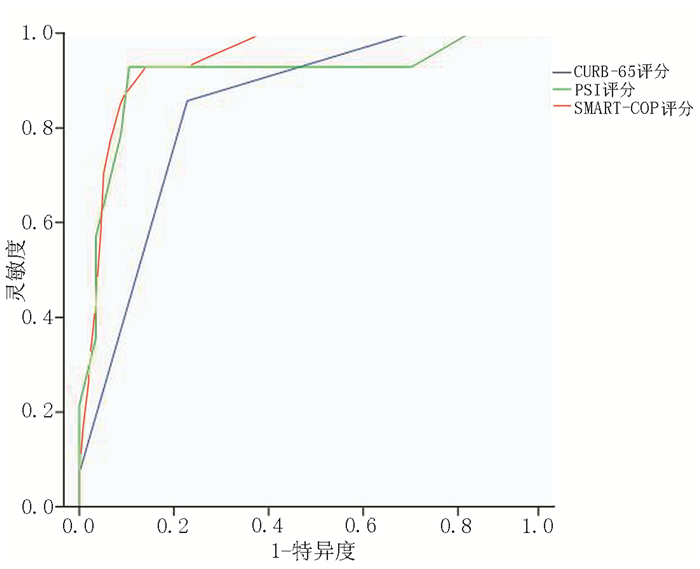
目的 比较PSI、CURB-65以及SMART-COP评分系统用于评估肾移植术后肺部感染严重程度和预测预后的价值。 方法 回顾性分析2009年1月至2015年6月西京医院收治的71例肾移植术后肺部感染患者的临床资料,其中重症感染组27例、非重症感染组44例。根据3种评分系统的危险分层标准将患者分成低危组和中、高危组。比较3种评分系统的不同危险分组患者的病死率、呼吸机使用率、重症监护室(ICU)入住率和住院时间。比较重症感染组与非重症感染组在3种评分系统中的得分差异。通过受试者工作特征(ROC)曲线比较3种评分系统预测患者肺部感染病死率的效能。 结果 在3种评分系统中,中、高危组患者的病死率、呼吸机使用率、ICU入住率较低危组明显升高(均为P < 0.05),所有中、高危组患者的住院时间均长于低危组(均为P<0.05)。重症感染组的PSI、CURB-65、SMART-COP评分的得分均明显高于非重症感染组(均为P<0.05)。PSI、CURB-65和SMART-COP评分评估死亡的最佳截点值分别为75分、1.5分和3.5分,其预测肾移植术后肺部感染病死率的灵敏度、特异度和曲线下面积(AUC)分别为0.929、0.890、0.909,0.857、0.772、0.844,0.929、0.860、0.941。 结论 PSI、CURB-65及SMART-COP评分均能反映肾移植术后肺部感染患者的病情严重程度和预测病死率,其中SMART-COP预测患者的病死率最准确,而PSI灵敏度高但操作复杂,CURB-65应用简单、方便。 Abstract:Objective To compare the performance of PSI, CURB-65 and SMART-COP systems in evaluating the severity and predicting the prognosis of pulmonary infection after renal transplantation. Methods Clinical data of 71 patients with pulmonary infection after renal transplantation in Xijing Hospital from January 2009 to June 2015 were retrospectively analyzed. All patients were divided into the severe (n=27) and mild infection groups (n=44). According to the risk-stratification criteria of three scoring systems, all patients were assigned into the low-risk group and moderate-high risk group. The fatality rate, utilization rate of respirator, occupancy rate of intensive care unit (ICU) and length of hospital stay were statistically compared among different risk groups of three scoring systems. The differences among the scores of three systems were compared between the severe and mild infection groups. The efficacy of three scoring systems in predicting the fatality rate of pulmonary infection patients was assessed by receiver operating characteristic (ROC) curve. Results By using three scoring systems, the fatality rate, utilization rate of respirator and occupancy rate of ICU in the moderate-high risk groups were significantly higher than those in the low-risk group (all P < 0.05). The length of hospital stay in the moderate-high risk group was significantly longer than that in the low-risk group (P < 0.05). The scores of PSI, CURB-65 and SMART-COP systems in the severe infection group were considerably higher than those in the mild infection group (all P < 0.05). The optimal cut-off scores of PSI, CURB-65 and SMART-COP systems were 75, 1.5 and 3.5, respectively. The sensitivity, specificity and AUC of PSI, CURB-65 and SMART-COP systems in predicting the fatality rate were calculated as 0.929, 0.890, 0.909; 0.857, 0.772, 0.844; 0.929, 0.860, 0.941, respectively. Conclusions PSI, CURB-65 and SMART-COP systems can assess the severity of pulmonary infection and predict the fatality rate after renal transplantation. SMART-COP possesses the highest accuracy in predicting the fatality rate. PSI is most sensitive but difficult to implement. CURB-65 is simple and convenient to apply in clinical practice. -
Key words:
- Renal transplantation /
- Pulmonary infection /
- Pulmonary infection scoring system /
- PSI /
- CURB-65 /
- SMART-COP
-

图 1 3种评分系统预测肾移植术后肺部感染病死率的ROC曲线
Figure 1. The ROC curve to evaluate 3 kinds of scaling systems on the mortality of pulmonary infection after renal transplantation
表 1 各评分系统不同危险分层的病死率、呼吸机使用率、ICU入住率及住院时间
Table 1. Mortality rates, ventilator frequency, ICU occupancy, and length of stay of each scaling system[n(%)]
评分系统 n 死亡 使用呼吸机 入住ICU 住院时间(x±s, d) PSI 低危组 59 5(9) 10(17) 4(7) 16±10 中、高危组 12 9(75)a 11(92)a 5(42)a 26±14a CURB-65 低危组 46 2(4) 3(7) 0(0) 14±10 160中、高危组 25 12(48)a 18(72)a 9(36)a 24±11a SMART-COP 低危组 45 1(2) 0(0) 0(0) 13±9 中、高危组 26 13(50)a 21(81)a 9(35)a 25±13a 注:与同一系统评分的低危组比较,aP<0.05  下载: 导出CSV
下载: 导出CSV
-
[1] Shih CJ, Tarng DC, Yang WC, et al. Immunosuppressant dose reduction and long-term rejection risk in renal transplant recipients with severe bacterial pneumonia [J]. Singapore Med J, 2014, 55(7):372-377. doi: 10.11622/smedj.2014089 [2] Marti C, Garin N, Grosgurin O, et al. Prediction of severe community-acquired pneumonia: a systematic review and meta-analysis [J]. Crit Care, 2012, 16(4):R141. doi: 10.1186/cc11447 [3] Froes F. PSI, CURB-65, SMART-COP or SCAP? and the winner is… SMART doctors [J]. Rev Port Pneumol, 2013, 19(6):243-244. doi: 10.1016/j.rppneu.2013.10.002 [4] Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults [J]. Clin Infect Dis, 2007, 44(2):S27-S72. http://www.medscape.com/medline/abstract/17278083 [5] Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study [J]. Thorax, 2003, 58(5): 377-382. doi: 10.1136/thorax.58.5.377 [6] Charles PG, Wolfe R, Whitby M, et al. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia [J]. Clin Infect Dis, 2008, 47(3): 375-384. doi: 10.1086/591413 [7] Zeynelogğlu P. Respiratory complications after solid-organ transplantation[J]. Exp Clin Transplant, 2015, 13(2): 115-125. https://www.researchgate.net/publication/274964406_Respiratory_Complications_After_Solid-Organ_Transplantation [8] Li JJ. Report: clinical characteristics and treatment experience report of severe pulmonary infection after renal transplantation [J]. Pak J Pharm Sci, 2015, 28(4):1559-1562. http://www.pjps.pk/wp-content/uploads/pdfs/28/4/Supplementary/21-SUP-284-Report.pdf [9] Masson P, Henderson L, Chapman JR, et al. Belatacept for kidney transplantation recipients[J]. Cochrane Database Syst Rev, 2014, 11:CD010699. [10] Serisier DJ, Williams S, Bowler SD. Australasian respiratory and emergency physicians do not use the pneumonia severity index in community-acquired pneumonia [J]. Respirology, 2013, 18(2): 291-296. doi: 10.1111/j.1440-1843.2012.02275.x [11] Ribeiro C, Ladeira I, Gaio AR, et al. Pneumococcal pneumonia: are the new severity scores more accurate in predicting adverse outcomes?[J]. Rev Port Pneumol, 2013, 19(6):252-259. doi: 10.1016/j.rppneu.2012.09.006 [12] Kwok CS, Loke YK, Woo K, et al. Risk prediction models for mortality in community-acquired pneumonia: a systematic review [J].Biomed Res Int, 2013: 504136. [13] Dizdar OS, Ersoy A, Akalin H. Pneumonia after kidney transplant: incidence, risk factors, and mortality [J]. Exp Clin Transplant, 2014, 12(3): 205-211. [14] 李文浩, 苏泽轩, 叶泽兵, 等.肾移植术后肺部感染预后的Cox风险模型分析[J].器官移植, 2015, 6(3): 179-183. http://www.organtranspl.com/browse/detail/qkid/88/id/122.htmlLi WH, Su ZX, Ye ZB, et al. Analysis on prognosis of pulmonary infection after renal transplantation by Cox risk model[J]. Organ Transplant, 2015, 6(3): 179-183. http://www.organtranspl.com/browse/detail/qkid/88/id/122.html [15] Ugajin M, Yamaki K, Iwamura N, et al. Blood urea nitrogen to serum albumin ratio independently predicts mortality and severity of community-acquired pneumonia [J].Int J Gen Med. 2012, 5: 583-589. http://www.docin.com/p-484485634.html [16] Naderi HR, Sheybani F, Sarvghad M, et al. Can procalcitonin add to the prognostic power of the severity scoring system in adults with pneumonia?[J]. Tanaffos, 2015, 14(2): 95-106. https://www.researchgate.net/profile/Fereshte_Sheybani2/publication/282611911_Can_Procalcitonin_Add_to_the_Prognostic_Power_of_the_Severity_Scoring_System_in_Adults_with_Pneumonia/links/5613fd5408aed47facedfbb2.pdf?origin=publication_detail -

 下载:
下载:

 点击查看大图
点击查看大图
图(1) / 表(1)
计量
- 文章访问数: 190
- HTML全文浏览量: 88
- PDF下载量: 6
- 被引次数: 0


