

Influence of sirolimus based triple anti-tumor therapy on T lymphocyte of rat model with liver cancer recurrence after transplantation
-
摘要:
目的 探讨以西罗莫司为基础联合槐耳颗粒、胸腺肽α-1的三联抗肿瘤疗法对大鼠肝癌肝移植复发模型T淋巴细胞的影响。 方法 72只Sprague-Dawley(SD)大鼠以随机数字法分为三联组、西罗莫司组、槐耳组、胸腺肽组、阳性对照组、空白组, 每组12只。除空白组外, 其余各组均采用化学诱癌法建立模拟肝癌肝移植术后复发的动物模型。模型建立后, 取阳性对照组大鼠鉴定模型是否成功建立。采用流式细胞术分别检测各组大鼠外周血调节性T细胞(Treg)占CD4+T淋巴细胞比例(Treg%)、CD4+T淋巴细胞占淋巴细胞总数比例(CD4+T%)及CD8+T淋巴细胞占淋巴细胞总数比例(CD8+T%)。采用Spearman秩相关分析Treg%与CD4+T%、CD8+T%及CD4+/CD8+T淋巴细胞比值(CD4+/CD8+)之间的关系。 结果 大鼠肝癌组织病理切片提示建模成功。阳性对照组的Treg%高于空白组, 差异有统计意义(P<0.05)。三联组的Treg%明显低于阳性对照组、胸腺肽组和槐耳组, 明显高于空白组(均为P<0.05)。与阳性对照组比较, 三联组、西罗莫司组和胸腺肽组的CD4+T%和CD8+T%较高, 差异有统计学意义(均为P<0.05)。三联组的CD4+T%和CD8+T%均高于胸腺肽组、西罗莫司组和槐耳组, 差异有统计学意义(均为P<0.05)。各组大鼠的外周血Treg%与CD4+ T%、CD8+ T%和CD4+/CD8+均呈负相关, 且三联抗肿瘤疗法可降低Treg%与CD4+/CD8+之间的负性相关关系。 结论 西罗莫司为基础的三联抗肿瘤疗法可降低大鼠外周血Treg水平, 提高T淋巴细胞数量及CD4+/CD8+, 发挥抗肿瘤细胞生长和增殖的作用。 Abstract:Objective To explore the influence of triple anti-tumor therapy which bases on sirolimus combined huaier granule and thymosin α-1 on T lymphocyte of rat model with liver cancer recurrence after transplantation. Methods Seventy-two Sprague-Dawley(SD)rats were randomly divided into triple therapy group, sirolimus group, huaier-granule group, thymosin α-1 group, positive-control group and blank group(n=12 in each group). Except the blank group, rats in all the other groups were established the simulation animal model of liver cancer recurrence after liver transplantation by chemical-induced method. After the model was established, rats in the positive control group were executed to appraise whether the model was successful. The proportion of regulatory T cells (Treg) of CD4+ T lymphocytes in peripheral blood (Treg%), the percentage of CD4+ T lymphocyte of total lymphocyte(CD4+T%)and the percentage of CD8+ T lymphocyte of total lymphocyte (CD8+T%), were detected by the flow cytometry respectively. The relationship between Treg% and CD4+ T%, CD8+ T%, the ratio of CD4+/CD8+ T lymphocytes(CD4+/CD8+)was analyzed by the method of Spearman rank correlation. Results Pathological section of rat liver tissue suggested that the rat model was established successfully. Treg% of positive control group was higher than that of blank group, the difference had statistical significance(P<0.05). Treg% of triple therapy group was significantly lower than that of the positive control group, huaier-granule group, thymosin α-1 group, and significantly higher than the blank group(all in P<0.05). Compared with positive-control group, CD4+T% and CD8+T% of triple therapy group, sirolimus group and thymosin α-1 group were significantly higher (all in P<0.05). CD4+T% and CD8+T% of triple therapy group were significantly higher than those of thymosin α-1 group, sirolimus group and huaier-granule group (all in P<0.05). The relationship between Treg% and CD4+T%, CD8+T%, CD4+/CD8+ in peripheral blood were negatively correlated for rats in each group. In addition, the triple anti-tumor therapy decreased the negative correlation between Treg% and CD4+/CD8+. Conclusions Sirolimus based triple anti-tumor therapy can decrease the peripheral blood Treg level of the liver cancer rat, increase the number of T lymphocyte and CD4+/CD8+, and play the role of anti tumor cell growth and proliferation. -
Key words:
- Sirlimus /
- Huaier /
- Thymosin α-1 /
- Tumor recurrence /
- Regulatory T cells /
- Liver transplantation /
- Cellular immunity
-

图 1 大鼠建模后的肝癌组织病理切片(HE)
注:A图放大倍数为200倍;B图放大倍数为400倍
Figure 1. Pathological section of liver cancer tissue of the model rats

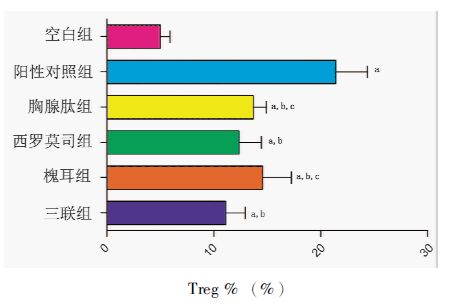
图 2 各组大鼠外周血Treg%的比较
注:与空白组比较,aP<0.05;与阳性对照组比较,bP<0.05;与三联组比较,cP<0.05
Figure 2. Comparison of Treg% in peripheral blood of rats among each group

图 3 各组大鼠外周血CD4+T%的比较
注:与阳性对照组比较,aP<0.05;与三联组比较,bP<0.05
Figure 3. Comparison of CD4+T% in peripheral blood of rats among each group

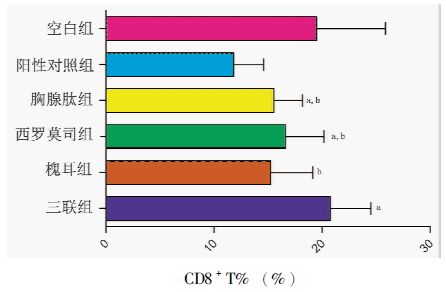
图 4 各组大鼠外周血CD8+T%的比较
注:与阳性对照组比较,aP<0.05;与三联组比较,bP<0.05
Figure 4. Comparison of CD8+T% in peripheral blood of rats among each group
表 1 各组大鼠Treg%与CD4+T%、CD8+T%、 CD4+/CD8+的相关性分析
Table 1. Correlation analysis between Treg% and CD4+T%, CD8+T%, CD4+/CD8+ among each group of rats
组别 Treg%与CD4+T% Treg%与CD8+T% Treg%与CD4+/CD8+ r P r P r P 三联组 -0.979 0 -0.955 0 -0.884 0.002 槐耳组 -0.908 0.033 -0.985 0.002 -0.897 0.039 西罗莫司组 -0.977 0 -0.946 0.001 -0.906 0.005 胸腺肽组 -0.931 0.021 -0.978 0.004 -0.945 0.015 阳性对照组 -0.998 0 -0.947 0.001 -0.964 0 空白组 -0.935 0 -0.648 0.043 -0.972 0  下载: 导出CSV
下载: 导出CSV
-
[1] Venook AP, Papandreou C, Furuse J, et al. The incidence and epidemiology of hepatocellular carcinoma: a global and regional perspective[J]. Oncologist, 2010, 15(Suppl 4):5-13. http://cn.bing.com/academic/profile?id=2145595073&encoded=0&v=paper_preview&mkt=zh-cn [2] Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma[J]. Lancet, 2012, 379(9822):1245-1255. doi: 10.1016/S0140-6736(11)61347-0 [3] Jemal A, Bray F, Center MM, et al. Global cancer statistics[J]. CA Cancer J Clin, 2011, 61(2):69-90. doi: 10.3322/caac.v61:2 [4] Llovet JM, Schwartz M, Mazzaferro V. Resection and liver transplantation for hepatocellular carcinoma[J]. Semin Liver Dis, 2005, 25(2):181-200. doi: 10.1055/s-2005-871198 [5] Bruix J, Sherman M, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma:an update[J]. Hepatology, 2011, 53(3):1020-1022. doi: 10.1002/hep.24199 [6] Davis E, Wiesner R, Valdecasas J, et al. Treatment of recurrent hepatocellular carcinoma after liver transplantation[J]. Liver Transpl, 2011, 17(Suppl 2):S162-S166. http://cn.bing.com/academic/profile?id=2077626674&encoded=0&v=paper_preview&mkt=zh-cn [7] Park MS, Lee KW, Suh SW, et al. Living-donor liver transplantation associated with higher incidence of hepatocellular carcinoma recurrence than deceased-donor liver transplantation[J]. Transplantation, 2014, 97(1):71-77. doi: 10.1097/TP.0b013e3182a68953 [8] Sharma P, Welch K, Hussain H, et al. Incidence and risk factors of hepatocellular carcinoma recurrence after liver transplantation in the MELD era[J]. Dig Dis Sci, 2012, 57(3):806-812. doi: 10.1007/s10620-011-1910-9 [9] Welker MW, Bechstein WO, Zeuzem S, et al. Recurrent hepatocellular carcinoma after liver transplantation: an emerging clinical challenge[J]. Transpl Int, 2013, 26(2):109-118. doi: 10.1111/tri.2013.26.issue-2 [10] Matter MS, Decaens T, Andersen JB, et al. Targeting the mTOR pathway in hepatocellular carcinoma: current state and future trends[J]. J Hepatol, 2014, 60(4):855-865. doi: 10.1016/j.jhep.2013.11.031 [11] Cholongitas E, Mamou C, Rodríguez-Castro KI, et al. Mammalian target of rapamycin inhibitors are associated with lower rates of hepatocellular carcinoma recurrence after liver transplantation: a systematic review[J]. Transpl Int, 2014, 27(10):1039-1049. doi: 10.1111/tri.2014.27.issue-10 [12] Liang W, Wang D, Ling X, et al. Sirolimus-based immunosuppression in liver transplantation for hepatocellular carcinoma: a meta-analysis[J]. Liver Transpl, 2012, 18(1):62-69. doi: 10.1002/lt.v18.1 [13] 杜国盛, 周林, 石炳毅, 等. 三联抗肿瘤疗法预防晚期原发性肝癌肝移植术后肿瘤复发的临床研究[J].器官移植, 2014, 5(2):74-78. http://www.cnki.com.cn/Article/CJFDTOTAL-QGYZ201402006.htmDu GS, Zhou L, Shi BY, et al. Clinical study of triple anti-tumor therapy for preventing tumor recurrence of terminal primary liver cancer after liver transplantation[J]. Organ Transplant, 2014, 5(2):74-78. http://www.cnki.com.cn/Article/CJFDTOTAL-QGYZ201402006.htm [14] 周林, 杜国盛, 朱志东, 等. 预防晚期肝内胆管细胞癌肝移植术后复发的三联疗法疗效报道[J/CD]. 中华普外科手术学杂志: 电子版, 2014, 8(1): 40-43.Zhou L, Du GS, Zhu ZD, et al. Prevention of recurrence of end-stage intrahepatic cholangiocellular carcinoma after liver transplantation by triple therapy[J/CD]. Chin J Oper Proc Gen Surg: Electronic Edition, 2014, 8(1): 40-43. [15] Thakur S, Singla A, Chawla Y, et al. Expansion of peripheral and intratumoral regulatory T cells in hepatocellular carcinoma: a case-control study[J]. Indian J Pathol Microbiol, 2011, 54(3):448-453. doi: 10.4103/0377-4929.85073 [16] Mathai AM, Kapadia MJ, Alexander J, et al. Role of Foxp3-positive tumor-infiltrating lymphocytes in the histologic features and clinical outcomes of hepatocellular carcinoma[J]. Am J Surg Pathol, 2012, 36(7):980-986. doi: 10.1097/PAS.0b013e31824e9b7c [17] 陈颖华, 蔡常洁, 陆敏强, 等.建立符合肝癌肝移植术后肝癌复发规律的大鼠模型[J].中山大学学报:医学科学版, 2006, 27(6):640-643. http://www.cnki.com.cn/Article/CJFDTOTAL-ZSYK200606013.htmChen YH, Cai CJ, Lu MQ, et al. A new rat model according with recrudescent mechanism after liver transplantation[J]. J Sun Yat-sen Univ: Medical Science, 2006, 27(6):640-643. http://www.cnki.com.cn/Article/CJFDTOTAL-ZSYK200606013.htm [18] Du Y, Chen X, Huang ZM, et al. Increased frequency of Foxp3+ regulatory T cells in mice with hepatocellular carcinoma[J]. Asian Pac J Cancer Prev, 2012, 13(8):3815-3819. doi: 10.7314/APJCP.2012.13.8.3815 [19] Lin SZ, Chen KJ, Xu ZY, et al. Prediction of recurrence and survival in hepatocellular carcinoma based on two Cox models mainly determined by FoxP3+ regulatory T cells[J]. Cancer Prev Res, 2013, 6(6):594-602. doi: 10.1158/1940-6207.CAPR-12-0379 [20] Sakaguchi S, Sakaguchi N, Asano M, et al. Pillars article: immunologic self-tolerance maintained by activated T cells expressing IL-2 receptor α-chains (CD25). breakdown of a single mechanism of self-tolerance causes various autoimmune diseases. J. Immunol. 1995[J]. J Immunol, 2011, 186(7):3808-3821. [21] Chen X, Du Y, Huang Z. CD4+ CD25+ Treg derived from hepatocellular carcinoma mice inhibits tumor immunity[J]. Immunol Lett, 2012, 148(1):83-89. doi: 10.1016/j.imlet.2012.09.002 [22] Lee WC, Wu TJ, Chou HS, et al. The impact of CD4+ CD25+ T cells in the tumor micro environment of hepatocellular carcinoma[J]. Surgery, 2012, 151(2):213-222. doi: 10.1016/j.surg.2011.07.029 [23] Huang Y, Liao H, Zhang Y, et al. Prognostic value of tumor-infiltrating FoxP3+ T cells in gastrointestinal cancers: a meta analysis[J]. PLoS One, 2014, 9(5):e94376. doi: 10.1371/journal.pone.0094376 -

 下载:
下载:


 点击查看大图
点击查看大图

计量
- 文章访问数: 125
- HTML全文浏览量: 17
- PDF下载量: 5
- 被引次数: 0


