

Application of multi-disciplinary team mode in prevention and control of multidrug resistant organism infection in lung transplant recipients
-
摘要:
目的 探讨多学科综合诊疗(MDT)模式在肺移植受者术后多重耐药菌(MDRO)感染防控中的实践效果。 方法 选择2019年至2022年的肺移植受者,从2020年1月开始成立MDT专家组,开展一系列防控措施,分析2020年至2022年MDRO防控措施落实率、环境物表MDRO检出率以及2019年至2022年肺移植受者MDRO检出率。 结果 医护人员总体MDRO防控措施落实率由2020年的64.9%上升至2022年的91.6%,呈逐年升高趋势(P<0.05)。监测环境物表MDRO检出率从2020年的28%下降到2022年的9%,呈逐年下降趋势(P<0.05)。肺移植受者MDRO检出率从2019年的66.7%降低至2022年的44.3%,呈逐年降低趋势(P<0.001)。 结论 通过MDT模式管理,提高了医务人员MDRO防控措施的执行力,有效降低了肺移植受者术后MDRO感染率和环境物表MDRO检出率,值得推广利用。 -
关键词:
- 肺移植 /
- 多重耐药菌 /
- 多学科综合诊疗 /
- 耐碳青霉烯类鲍曼不动杆菌 /
- 耐碳青霉烯类大肠埃希菌 /
- 耐碳青霉烯类肺炎克雷伯菌 /
- 耐甲氧西林金黄色葡萄球菌 /
- 耐碳青霉烯类铜绿假单胞菌
Abstract:Objective To evaluate the effectiveness of multi-disciplinary team (MDT) mode in the prevention and control of multidrug resistant organism (MDRO) infection in lung transplant recipients. Methods Lung transplant recipients admitted to the hospital from 2019 to 2022 were enrolled. MDT expert group was established in January, 2020. A series of prevention and control measures were conducted. The implementation rate of MDRO prevention and control measures and the detection rate of MDRO on the environmental surface from 2020 to 2022, and the detection rate of MDRO in lung transplant recipients from 2019 to 2022 were analyzed. Results The overall implementation rate of MDRO prevention and control measures for medical staff was increased from 64.9% in 2020 to 91.6% in 2022, showing an increasing trend year by year (P<0.05). The detection rate of MDRO on the environmental surface was decreased from 28% in 2020 to 9% in 2022, showing a downward trend year by year (P<0.05). The detection rate of MDRO in lung transplant recipients was decreased from 66.7% in 2019 to 44.3% in 2022, showing a decreasing trend year by year (P<0.001). Conclusions MDT mode management may enhance the implementation of MDRO prevention and control measures for medical staff, effectively reduce the infection rate of MDRO in lung transplant recipients and the detection rate of MDRO on the environmental surface, which is worthy of widespread application. -
Key words:
- Lung transplantation /
- Multidrug resistant organism /
- Multi-disciplinary team /
- Carbapenem-resistant acinetobacter baumannii /
- Carbapenem-resistant escherichia coli /
- Carbapenem-esistant Klebsiella pneumoniae /
- Methicillin-resistant Staphylococcus aureus /
- Carbapenem-resistant Pseudomonas aeruginosa
-

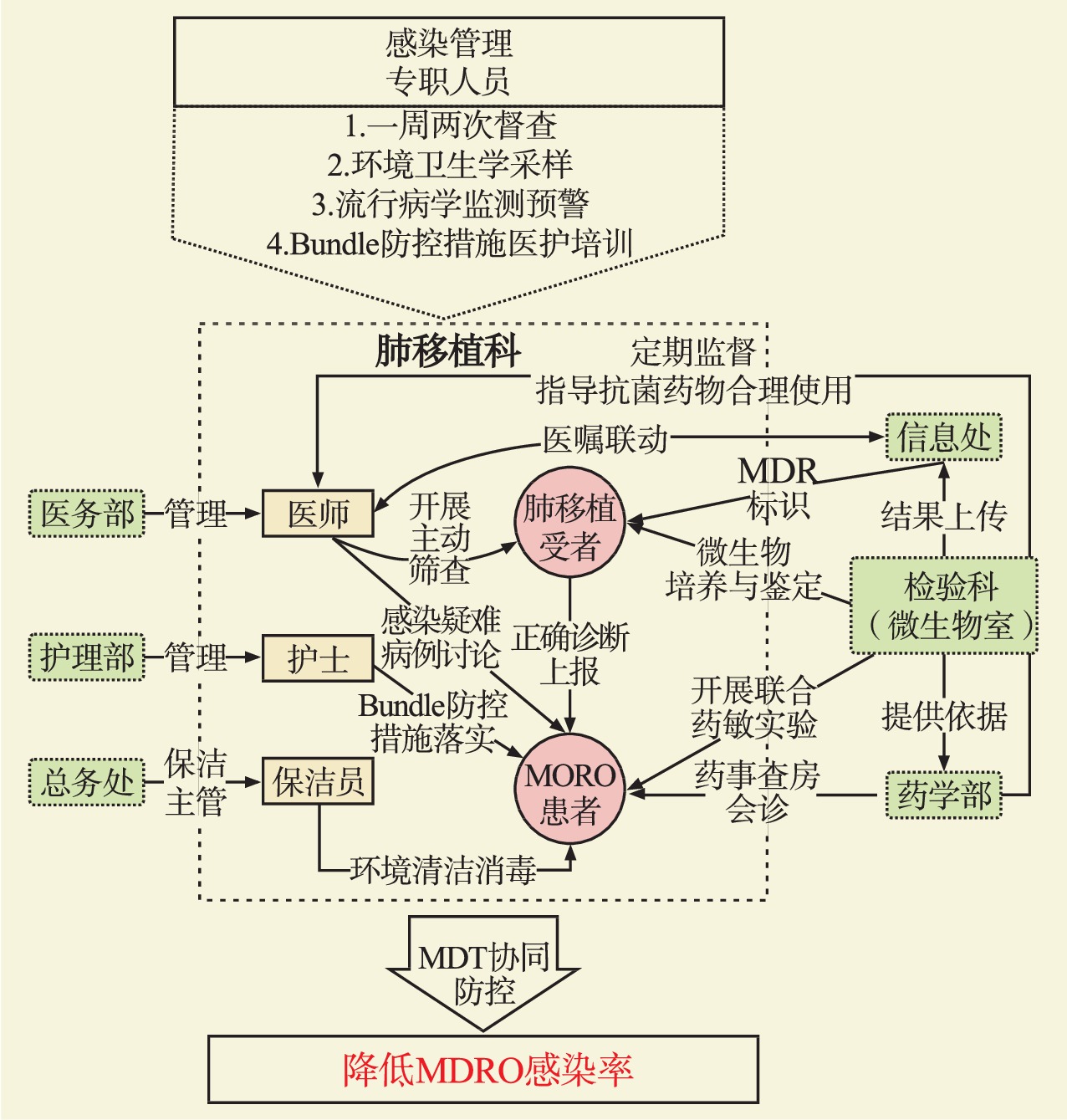
图 1 MDT对肺移植受者MDRO感染防控管理技术路线图
Figure 1. Roadmap of MDT for MDRO infection prevention and control management in lung transplant recipients
表 1 2020年至2022年MDRO防控措施落实率情况
Table 1. Implementation rate of MDRO prevention and control measures from 2020 to 2022
防控措施 2020年 2021年 2022年 χ2检验 趋势检验 执行数/应执行数 执行率(%) 执行数/应执行数 执行率(%) 执行数/应执行数 执行率(%) χ2值 P值 Z值 P值 总防控措施 721/1 111 64.9 858/1 093 78.5 104 7/1 143 91.6 237.71 <0.001 −15.41 <0.001 医生核心防控措施① 285/460 62.0 348/439 79.3 419/463 90.5 108.43 <0.001 −10.33 <0.001 护士核心防控措施② 436/651 67.0 510/654 78.0 628/680 92.3 131.50 <0.001 −11.43 <0.001 注:①医生核心防护措施包括接触隔离医嘱及时开具、手卫生依从、近距离操作防控、查房诊疗操作顺序正确、抗菌药物合理使用。
②护士核心防控措施包括单间/床边隔离、患者专用物品和隔离标识配备、患者及家属宣教、床单元环境清洁消毒、医用织物和医疗废物正确处置、手卫生依从、近距离操作防控。 下载: 导出CSV
下载: 导出CSV
表 2 2020年至2022年环境物表卫生学MDRO检出情况
Table 2. The detection of MDRO in environmental surface hygiene from 2020 to 2022
细菌名称 2020年 2021年 2022年 χ2检验 趋势检验 检出数/特定细菌数 检出率①(%) 检出数/特定细菌数 检出率①(%) 检出数/特定细菌数 检出率①(%) χ2值 P值 Z值 P值 MRSA 11/36 31 6/31 19 3/28 11 3.81 0.15 1.94 0.053 CRKP 5/35 14 2/15 13 0/9 1.43 0.49 0.70 0.485 CRAB 6/9 1/4 1/9 5.63 0.043 2.40 0.017 合计 22 28 9 18 4 9 6.41 0.04 2.57 0.01 注:①合计例数较少的(<10),不统计百分率。
下载: 导出CSV
表 3 2019年至2022年肺移植受者MDRO检出情况
Table 3. Detection of MDRO in lung transplant recipients from 2019 to 2022
细菌名称 2019年 2020年 2021年 2022年 χ2检验 趋势检验 检出数/特定细菌数 检出率(%) 检出数/特定细菌数 检出率(%) 检出数/特定细菌数 检出率(%) 检出数/特定细菌数 检出率(%) χ2值 P值 Z值 P值 CREC 4/11 36.4 3/17 17.6 3/15 20.0 2/25 8.0 4.3 0.230 1.87 0.062 CRKP 81/112 72.3 60/97 61.9 50/104 48.1 39/91 42.9 22.4 <0.001 4.67 <0.001 MRSA 16/30 53.3 11/31 35.5 13/40 32.5 9/38 23.7 6.7 0.084 2.46 0.014 CRAB 93/113 82.3 82/99 82.8 85/126 67.5 59/89 66.3 13.7 0.003 3.33 <0.001 CRPA 66/124 53.2 47/113 41.6 57/124 46.0 50/116 43.1 3.9 0.275 1.31 0.190 合计 260/390 66.7 203/357 56.9 208/409 50.9 159/359 44.3 46.4 <0.001 6.74 <0.001
下载: 导出CSV
-
[1] CHANG SH, CHAN J, PATTERSON GA. History of lung transplantation[J]. Clin Chest Med, 2023, 44(1): 1-13. DOI: 10.1016/j.ccm.2022.11.004. [2] LOOR G, MATTAR A, SCHAHEEN L, et al. Surgical complications of lung transplantation[J]. Thorac Surg Clin, 2022, 32(2): 197-209. DOI: 10.1016/j.thorsurg.2022.01.003. [3] JOEAN O, WELTE T, GOTTLIEB J. Chest infections after lung transplantation[J]. Chest, 2022, 161(4): 937-948. DOI: 10.1016/j.chest.2021.10.014. [4] 赵键. 多重耐药菌流行现状、耐药机制及其治疗策略[J]. 济宁医学院学报, 2023, 46(3): 216-220. DOI: 10.3969/j.issn.1000-9760.2023.03.014.ZHAO J. Current situation, resistance mechanisms and treatment strategies of multidrug-resistant bacteria[J]. J Jining Med Univ, 2023, 46(3): 216-220. DOI: 10.3969/j.issn.1000-9760.2023.03.014. [5] SY CL, CHEN PY, CHENG CW, et al. Recommendations and guidelines for the treatment of infections due to multidrug resistant organisms[J]. J Microbiol Immunol Infect, 2022, 55(3): 359-386. DOI: 10.1016/j.jmii.2022.02.001. [6] HONG NGUYEN M, SHIELDS RK, CHEN L, et al. Molecular epidemiology, natural history, and long-term outcomes of multidrug-resistant enterobacterales colonization and infections among solid organ transplant recipients[J]. Clin Infect Dis, 2022, 74(3): 395-406. DOI: 10.1093/cid/ciab427. [7] BEZINOVER D, BIANCOFIORE G, FALCONE M, et al. Multidrug-resistant infections in solid organ transplant recipients: a focus on risk factors, prevention, and treatment strategies[J]. Minerva Anestesiol, 2022, 88(9): 735-747. DOI: 10.23736/S0375-9393.22.16124-9. [8] WONG D, VAN DUIN D. Carbapenemase-producing organisms in solid organ transplantation[J]. Curr Opin Organ Transplant, 2019, 24(4): 490-496. DOI: 10.1097/MOT.0000000000000664. [9] VAN DUIN D, DOI Y. The global epidemiology of carbapenemase-producing Enterobacteriaceae[J]. Virulence, 2017, 8(4): 460-469. DOI: 10.1080/21505594.2016.1222343. [10] 黄丽华, 刘娇, 彭雪儿, 等. 2019~2021年某肿瘤专科医院院内感染情况分析[J]. 中山大学学报(医学科学版), 2023, 44(4): 697-703. DOI: 10.13471/j.cnki.j.sun.yat-sen.univ(med.sci).20230409.002.HUANG LH, LIU J, PENG XE, et al. Analysis of Nosocomial Infection in a Cancer Hospital from 2019 to 2021[J]. J Sun Yat-sen Univ (Med Sci), 2023, 44(4): 697-703. DOI: 10.13471/j.cnki.j.sun.yat-sen.univ(med.sci).20230409.002. [11] 陈美利, 景照峰, 黄合田, 等. 某三级综合医院多重耐药菌防控管理新模式探讨[J]. 中国感染控制杂志, 2023, 22(8): 925-931. DOI: 10.12138/j.issn.1671-9638.2023 4240.CHEN ML, JING ZF, HUANG HT, et al. A new management mode for the prevention and control of multidrug-resistant organisms in a tertiary hospital[J]. Chin J Infect Control, 2023, 22(8): 925-931. DOI: 10.12138/j.issn.1671-9638.20234240. [12] KANJ SS, BASSETTI M, KIRATISIN P, et al. Clinical data from studies involving novel antibiotics to treat multidrug-resistant Gram-negative bacterial infections[J]. Int J Antimicrob Agents, 2022, 60(3): 106633. DOI: 10.1016/j.ijantimicag.2022.106633. [13] BARBER KE, WAGNER JL, LARRY RC, et al. Frequency of and risk factors for carbapenem-resistant enterobacteriaceae[J]. J Med Microbiol, 2021, 70(2): 001286. DOI: 10.1099/jmm.0.001286. [14] DAWSON C, ROE J, STARMER H, et al. Patient advocacy in head and neck cancer: realities, challenges and the role of the multi-disciplinary team[J]. Clin Otolaryngol, 2020, 45(4): 437-444. DOI: 10.1111/coa.13508. [15] 商冠宁. 多学科综合诊疗协作组模式在骨肿瘤规范化诊疗中的应用[J]. 中国肿瘤外科杂志, 2022, 14(5): 417-420. DOI: 10.3969/j.issn.1674-4136.2022.05.001.SHANG GN. Application of MDT model in standardized diagnosis and treatment of bone tumors[J]. Chin J Surg Oncol, 2022, 14(5): 417-420. DOI: 10.3969/j.issn.1674-4136.2022.05.001. [16] 中国抗癌协会妇科肿瘤专业委员会, 中国抗癌协会肿瘤多学科诊疗(MDT)专业委员会, 中国医师协会肿瘤多学科诊疗专业委员会. 妇科恶性肿瘤多学科诊疗中国专家共识(2022年版)[J]. 中国癌症杂志, 2022, 32(8): 747-756. DOI: 10.19401/j.cnki.1007-3639.2022.08.010.The Society of Gynecological Cancer of China Anti-Cancer Association, Multidisciplinary Diagnosis and Treatment (MDT) Committee of China Anti-Cancer Association, Multidisciplinary Cancer Diagnosis and Treatment Committee of Chinese Medical Doctor Association. Consensus of Chinese experts on multidisciplinary team of gynecological malignant tumors (2022 edition)[J]. China Oncol, 2022, 32(8): 747-756. DOI: 10.19401/j.cnki.1007-3639.2022.08.010. [17] BOUCHAND F, DINH A, ROUX AL, et al. Implementation of a simple innovative system for postprescription antibiotic review based on computerized tools with shared access[J]. J Hosp Infect, 2017, 95(3): 312-317. DOI: 10.1016/j.jhin.2016.11.011. [18] JENKINS N, HUGHES H. How I do it…. how infection doctors approach the PJI MDT[J]. Knee, 2020, 27(6): 1994-1997. DOI: 10.1016/j.knee.2020.09.005. [19] 白镓玮, 马承泰, 吴淼, 等. 肺移植术后多重耐药菌感染的防治研究进展[J]. 武汉大学学报(医学版), 2021, 42(4): 551-557. DOI: 10.14188/j.1671-8852.2021.6010.BAI JW, MA CT, WU M, et al. Research progress in the prevention and treatment of multidrug-resistant organisms infection after lung transplantation[J]. Med J Wuhan Univ, 2021, 42(4): 551-557. DOI: 10.14188/j.1671-8852.2021.6010. [20] 蔡小军, 宋惠珠, 焦正, 等. 242例肺移植受者的感染病原菌分布及耐药特征分析[J]. 中华器官移植杂志, 2017, 38(9): 513-519. DOI: 10.3760/cma.j.issn.0254-1785.2017.09.001.CAI XJ, SONG HZ, JIAO Z, et al. Distribution and drug resistance characteristics of pathogens for infection after lung transplantation from 2010 to 2016[J]. Chin J Organ Transplant, 2017, 38(9): 513-519. DOI: 10.3760/cma.j.issn.0254-1785.2017.09.001. [21] 蔡虻, 刘聚源. 多重耐药菌医院感染防控策略与思考[J]. 中国护理管理, 2018, 18(12): 1590-1594. DOI: 10.3969/j.issn.1672-1756.2018.12.002.CAI M, LIU JY. Thinking on the strategy on prevention and control of Multidrug-Resistant Organism healthcare-associated infection[J]. Chin Nurs Manag, 2018, 18(12): 1590-1594. DOI: 10.3969/j.issn.1672-1756.2018.12.002. [22] 裴媛玲, 周丽清, 刘淑萍, 等. 多重耐药菌感染防控中全程标准化流程管理的构建及效果[J]. 基层医学论坛, 2023, 27(18): 123-125. DOI: 10.19435/j.1672-1721.2023. 18.039.PEI YL, ZHOU LQ, LIU SP, et al. Construction and effectiveness of standardized process management for the prevention and control of multidrug-resistant bacterial infections[J]. Med Forum, 2023, 27(18): 123-125. DOI: 10.19435/j.1672-1721.2023.18.039. [23] ABAD CL, BARKER AK, SAFDAR N. A systematic review of the effectiveness of cohorting to reduce transmission of healthcare-associated C. difficileand multidrug-resistant organisms[J]. Infect Control Hosp Epidemiol, 2020, 41(6): 691-709. DOI: 10.1017/ice.2020.45. [24] DOUGLAS AP, STEWART AG, HALLIDAY CL, et al. Outbreaks of fungal infections in hospitals: epidemiology, detection, and management[J]. J Fungi (Basel), 2023, 9(11): 1059. DOI: 10.3390/jof9111059. [25] 邓晓辉, 康亚辉, 贺锐, 等. 多层级多学科综合治疗模式对院内感染防控的结果分析[J]. 中国妇幼保健, 2022, 37(13): 2493-2496. DOI: 10.19829/j.zgfybj.issn.1001-4411.2022.13.045.DENG XH, KANG YH, HE R, et al. Analysis on the prevention and control effect of multi-level and multi-disciplinarity comprehensive treatment model on hospital infection[J]. Matern Child Health Care China, 2022, 37(13): 2493-2496. DOI: 10.19829/j.zgfybj.issn.1001-4411.2022.13.045. [26] 燕超, 齐金龙, 刘莉. 多学科协作在儿童多重耐药菌医院感染防控中的应用[J]. 生命科学仪器, 2022, 20(z1): 390. DOI: 10.11967/2022006166.YAN C, QI JL, LIU L. Application of multidisciplinary collaboration in hospital infection prevention and control of multidrug-resistant bacteria in children[J]. Life Sci Instrum, 2022, 20(z1): 390. DOI: 10.11967/2022006166. [27] KELLY BJ, BEKELE S, LOUGHREY S, et al. Healthcare microenvironments define multidrug-resistant organism persistence[J]. Infect Control Hosp Epidemiol, 2022, 43(9): 1135-1141. DOI: 10.1017/ice.2021.323. [28] PETERS A, SCHMID MN, PARNEIX P, et al. Impact of environmental hygiene interventions on healthcare-associated infections and patient colonization: a systematic review[J]. Antimicrob Resist Infect Control, 2022, 11(1): 38. DOI: 10.1186/s13756-022-01075-1. [29] CRUZ-LÓPEZ F, MARTÍNEZ-MELÉNDEZ A, VILLARREAL-TREVIÑO L, et al. Contamination of healthcare environment by carbapenem-resistant Acinetobacter baumannii[J]. Am J Med Sci, 2022, 364(6): 685-694. DOI: 10.1016/j.amjms.2022.07.003. [30] TENG J, IMANI S, ZHOU A, et al. Combatting resistance: understanding multi-drug resistant pathogens in intensive care units[J]. Biomed Pharmacother, 2023, 167: 115564. DOI: 10.1016/j.biopha.2023.115564. [31] USHIRO-LUMB I, THORBURN D. Risk of transmission of infections to others after donor-derived infection transmissions[J]. Transpl Infect Dis, 2022, 24(2): e13791. DOI: 10.1111/tid.13791. [32] ZHOU WY, SHEN L, SHI JX, et al. Real-time, random-access organ screening for carbapenem-resistant organisms (CRO) reduces CRO-associated, donor-derived infection mortality in lung transplant recipients[J]. Infection, 2023,DOI: 10.1007/s15010-023-02089-6[Epub ahead of print]. [33] DOĞAN KAYA S, TAŞÇI E, KIRALI K. Evaluation of donor-derived bacterial infections in lung transplant recipients[J]. Turk Gogus Kalp Damar Cerrahisi Derg, 2023, 31(2): 269-274. DOI: 10.5606/tgkdc.dergisi.2023.23489. [34] 中华医学会器官移植学分会, 中华预防医学会医院感染控制学分会, 复旦大学华山医院抗生素研究所. 中国实体器官移植供者来源感染防控专家共识(2018版)[J]. 中华器官移植杂志, 2018, 39(1): 41-52. DOI: 10.3760/cma.j.issn.0254-1785.2018.01.008.Organ Transplantation Branch of Chinese Medical Association, Healthcare-Associated Infection Control of Chinese Preventive Medicine Association, Institute of Antibiotics of Huashan Hospital, Fudan University. The consensus on donor-derived infection control of solid organ transplantation in China(2018)[J]. Chin J Organ Transplant, 2018, 39(1): 41-52. DOI: 10.3760/cma.j.issn.0254-1785.2018.01.008. [35] ANESI JA, BLUMBERG EA, HAN JH, et al. Impact of donor multidrug-resistant organisms on solid organ transplant recipient outcomes[J]. Transpl Infect Dis, 2022, 24(1): e13783. DOI: 10.1111/tid.13783. [36] TEBANO G, GENEVE C, TANAKA S, et al. Epidemiology and risk factors of multidrug-resistant bacteria in respiratory samples after lung transplantation[J]. Transpl Infect Dis, 2016, 18(1): 22-30. DOI: 10.1111/tid.12471. [37] CARILLO C, PECORARO Y, ANILE M, et al. Colistin-based treatment of multidrug-resistant gram-negative bacterial pulmonary infections after lung transplantation[J]. Transplant Proc, 2019, 51(1): 202-205. DOI: 10.1016/j.transproceed.2018.04.068. [38] 聂俊, 朱颖, 江波. 肺癌多学科协作存在的问题及对策[J]. 医学与哲学, 2018, 39(16): 4-6. DOI: 10.12014/j.issn.1002-0772.2018.08b.02.NIE J, ZHU Y, JIANG B. The problems and solutions of lung cancer MDT[J]. Med Philos, 2018, 39(16): 4-6. DOI: 10.12014/j.issn.1002-0772.2018.08b.02. -

 下载:
下载:

 点击查看大图
点击查看大图
计量
- 文章访问数: 22
- HTML全文浏览量: 8
- PDF下载量: 2
- 被引次数: 0


