

Clinical and epidemiological features analysis of pneumocystis jirovecii pneumonia in kidney transplant recipients
-
摘要:
目的 探讨肾移植受者耶氏肺孢子菌肺炎(PJP)的临床及流行病学特征。 方法 收集2021年7月至2021年12月68例肾移植受者的临床资料,根据肺部感染情况分为PJP组(11例)、普通肺部感染组(24例)、非肺炎组(33例)。分析肾移植术后PJP的发生及治疗情况,比较各组受者的基本特征及实验室指标,分析PJP患者的基因分型及传播图谱。 结果 64例肾移植受者中,11例明确诊断PJP,最常见的临床表现为体温升高、干咳伴进行性呼吸困难。所有患者胸部CT表现为双肺弥漫性间质炎症,磨玻璃样改变。确诊后,均口服复方磺胺甲 结论 由于细胞免疫功能受损,肾移植受者更易感染耶式肺孢子菌(PJ),最常见的临床表现为体温升高、干咳伴进行性呼吸困难,部分同时出现头痛,乏力,胸部CT表现为双肺弥漫性间质炎症、磨玻璃样改变。PJ可通过呼吸道传播,在肾移植随访门诊存在小规模的PJP爆发可能,应及时做好预防工作。 Abstract:Objective To investigate clinical and epidemiological features of pneumocystis jirovecii pneumonia (PJP) in kidney transplant recipients. Methods Clinical data of 68 kidney transplant recipients admitted from July, 2021 to December, 2021 were collected. All patients were divided into the PJP group (n=11), common pulmonary infection group (n=24) and non-pneumonia group (n=33) according to the status of pulmonary infection. The incidence and treatment of PJP after kidney transplantation were analyzed. Basic characteristics and laboratory parameters of the recipients were compared among all groups. The genotyping and transmission map of PJP patients were evaluated. Results Among 64 kidney transplant recipients, 11 cases were definitely diagnosed with PJP. The most common clinical manifestations included elevated body temperature, and dry cough complicated with progressive dyspnea. Chest CT scan showed diffuse interstitial inflammation and ground glass-like lesions of bilateral lungs in all patients. After diagnosis, all patients were orally given with compound sulfamethoxazole for 3-4 weeks. Two patients received non-invasive ventilator-assisted ventilation due to severe lung infection and dyspnea, and the remaining patients were given with nasal cannula oxygenation. One patient experienced elevated serum creatinine level upon discharge, and developed renal allograft failure. The remaining 10 recipients with PJP obtained normal renal allograft function, and no recipient died. Compared with the non-pneumonia group, the rejection rate was higher, the length of hospital stay was longer, the lymphocyte count was less, the lymphocyte proportion was lower, the levels of C-reactive protein, serum creatinine and lactate dehydrogenase were higher, and the levels of serum albumin was lower and CD4+T cell count was less in the PJP group (all P < 0.05). Compared with common pulmonary infection group, the lymphocyte count was less, the lymphocyte proportion was lower, the CD4+T cell count was less and 1, 3-β-D- glucan (BDG) level was higher in the PJP group (all P < 0.05). No new genotype was detected in 10 of the 12 testing samples. It was considered that PJP mainly depended on two transmission chains and two independent transmission individuals. Conclusions Kidney transplant recipients are prone to pneumocystis jirovecii (PJ) infection due to impaired cellular immune function. The most common clinical manifestations consist of elevated body temperature and dry cough complicated with progressive dyspnea, accompanied by headache and fatigue in partial patients. Chest CT scan shows diffuse interstitial inflammation and ground glass-like lesion of bilateral lungs. PJ may be transmitted through respiratory tract. Small-scale PJP might occur in the follow-up outpatient of kidney transplant recipients. Preventive measures should be delivered in a timely manner. -

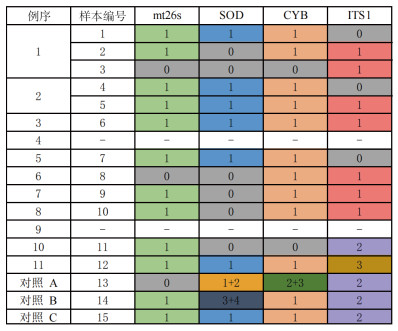
图 1 11例患者的样本检测结果
注:PCR+Sanger测序阴性的基因用0表示,PCR+Sanger测序阳性基因,当来源于同一进化树分支时用相同的数字表示,当1个样本中同时检测出多种不同基因分型则用不同数字组合表示。
Figure 1. Sample test results of 11 patients
表 1 PJP患者病原学诊断结果
Table 1. Pathogenic test results of patients with PJP
例序 mNGS样本类型 mNGS结果 痰培养 血培养 CMV DNA 细菌 病毒 真菌 1 血液/尿液 阴性 阴性 PJ 阴性 阴性 阴性 2 肺泡灌洗液 阴性 阴性 PJ 阴沟肠杆菌属 阴性 阴性 3 肺泡灌洗液 阴性 阴性 PJ 未做 阴性 未做 4 肺泡灌洗液 阴性 阴性 PJ 阴性 阴性 阴性 5 肺泡灌洗液 阴性 乙型肝炎病毒 PJ 阴性 未做 阴性 6 肺泡灌洗液 嗜血杆菌 阴性 PJ 阴性 未做 阴性 7 肺泡灌洗液 副流感嗜血杆菌
肺炎链球菌人疱疹病毒-1 PJ 阴性 未做 阴性 8 肺泡灌洗液 副流感嗜血杆菌
肺炎克雷伯菌
肺炎链球菌阴性 PJ 阴性 未做 未做 9 肺泡灌洗液 阴性 阴性 PJ 阴性 未做 未做 10 肺泡灌洗液 纹带棒状杆菌
粪肠球菌
铜绿假单胞菌阴性 PJ 未做 未做 未做 11 肺泡灌洗液 纹带棒状杆菌 CMV PJ 阴性 阴性 阴性  下载: 导出CSV
下载: 导出CSV
表 2 3组受者的基本特征及实验室结果比较
Table 2. Comparison of basic characteristics and laboratory results of recipients among 3 groups
变量 PJP组
(n=11)普通肺部感染组
(n=24)非肺炎组
(n=33)统计值 P值 男性[n(%)] 7(64) 13(54) 22(67) 0.939 0.625 年龄(x±s,岁) 46±7 52±10 44±10b 5.470 0.006 服用他克莫司[n(%)] 10(91) 14(58) 27(82) 6.962 0.269 排斥反应[n(%)] 2(18) 2(8) 0a 5.224 0.046 术后肺部感染时间[M(P25, P75),月] 15(8,24) 30(12,48) -① 84.500 0.088 住院时间[M(P25, P75),d] 12(10,19) 9(7,13) 3(3,3)a, b 52.208 < 0.001 C-反应蛋白[M(P25, P75),mg/L] 21.47(16.94,42.06) 44.60(12.10,69.55) 1.16(0.22,3.01)a, b 43.673 < 0.001 降钙素原[M(P25, P75),ng/mL] 0.07(0.04,0.17) 0.04(0.03,0.07) - 89.000 0.114 白细胞计数[M(P25, P75),×109/L] 7.14(6.43,9.80) 6.76(5.15,8.84) 7.58(6.67,9.31) 1.324 0.516 淋巴细胞计数[M(P25, P75),×109/L] 0.59(0.24,0.72) 0.85(0.46,1.20)a 1.07(0.93,1.26)a, b 21.663 < 0.001 淋巴细胞比例[M(P25, P75),%] 6.8(2.50,10.40 11.0(9.20,19.00)a 14.6(10.85,17.50)a 17.034 < 0.001 血清肌酐[M(P25, P75),μmol/L] 156(125,184) 133(112,192) 93(75,106)a, b 22.857 < 0.001 乳酸脱氢酶[M(P25, P75),U/L] 288(236,402) 232(192,333) 174(158,192)a, b 26.645 < 0.001 血清白蛋白[M(P25, P75),g/L] 30.5(26.8,37.9) 36.1(33.3,39.6) 40.9(38.0,43.4)a, b 16.884 < 0.001 血钙[M(P25, P75),mmol/L] 2.30(2.17,2.47) 2.34(2.20,2.52) 2.38(2.28,2.49) 1.909 0.385 血钠[M(P25, P75),mmol/L] 138(137,140) 141(139,142) 141(140,142)a 9.447 0.009 CD4+T细胞计数[M(P25, P75),/μL] 142(88,349) 386(275,699)a 503(315,702)a 13.108 0.001 CD4/CD8[M(P25, P75)] 1.60(1.20,2.80) 1.45(0.83,1.96) 1.30(0.80, 1.65) 2.610 0.271 BDG≥37 pg/mL[n(%)] 8(73) 3(13)a - 10.055 0.002 注:与PJP组比较,aP < 0.05;与普通肺部感染组比较,bP < 0.05;组间比较为Bonferroni校正P值。
①-为无数据。
下载: 导出CSV
-
[1] HOSSEINI-MOGHADDAM SM, OUÉDRAOGO A, NAYLOR KL, et al. Incidence and outcomes of invasive fungal infection among solid organ transplant recipients: a population-based cohort study[J]. Transpl Infect Dis, 2020, 22(2): e13250. DOI: 10.1111/tid.13250. [2] APOSTOLOPOULOU A, FISHMAN JA. The pathogenesis and diagnosis of pneumocystis jiroveci pneumonia[J]. J Fungi (Basel), 2022, 8(11): 1167. DOI: 10.3390/jof8111167. [3] HOSSEINI-MOGHADDAM SM, SHOKOOHI M, SINGH G, et al. Six-month risk of pneumocystis pneumonia following acute cellular rejection: a case-control study in solid organ transplant recipients[J]. Clin Transplant, 2021, 35(7): e14322. DOI: 10.1111/ctr.14322. [4] ZHANG F, CHEN J, HUANG H, et al. Application of metagenomic next-generation sequencing in the diagnosis and treatment guidance of pneumocystis jirovecii pneumonia in renal transplant recipients[J]. Eur J Clin Microbiol Infect Dis, 2021, 40(9): 1933-1942. DOI: 10.1007/s10096-021-04254-x. [5] XIE D, XU W, YOU J, et al. Clinical descriptive analysis of severe pneumocystis jirovecii pneumonia in renal transplantation recipients[J]. Bioengineered, 2021, 12(1): 1264-1272. DOI: 10.1080/21655979.2021.1911203. [6] XU J, YU Y, LV J, et al. Application of metagenomic next-generation sequencing to diagnose pneumocystis jirovecii pneumonia in kidney transplantation recipients[J]. Ann Transplant, 2021, 26: e931059. DOI: 10.12659/AOT.931059. [7] DE BOER MG, DE FIJTER JW, KROON FP. Outbreaks and clustering of pneumocystis pneumonia in kidney transplant recipients: a systematic review[J]. Med Mycol, 2011, 49(7): 673-680. DOI: 10.3109/13693786.2011.571294. [8] LE GAL S, TOUBAS D, TOTET A, et al. Pneumocystis infection outbreaks in organ transplantation units in France: a nation-wide survey[J]. Clin Infect Dis, 2020, 70(10): 2216-2220. DOI: 10.1093/cid/ciz901. [9] RICCI G, SANTOS DW, KOVACS JA, et al. Genetic diversity of pneumocystis jirovecii from a cluster of cases of pneumonia in renal transplant patients: cross-sectional study[J]. Mycoses, 2018, 61(11): 845-852. DOI: 10.1111/myc.12823. [10] MAITTE C, LETERRIER M, LE PAPE P, et al. Multilocus sequence typing of pneumocystis jirovecii from clinical samples: how many and which loci should be used?[J]. J Clin Microbiol, 2013, 51(9): 2843-2849. DOI: 10.1128/JCM.01073-13. [11] 韩嘉静, 赵建康, 刘鑫梦, 等. 耶氏肺孢子菌肺炎临床特征分析[J]. 中华检验医学杂志, 2022, 45(9): 930-935. DOI: 10.3760/cma.j.cn114452-20211108-00689.HAN JJ, LIU JK, LIU XM, et al. Clinical features of pneumocystis jirovecii pneumonia[J]. Chin J Lab Med, 2022, 45(9): 930-935. DOI: 10.3760/cma.j.cn114452-20211108-00689. [12] 薛婷, 杜伟勤. 耶氏肺孢子菌基因分型研究进展[J]. 中国寄生虫学与寄生虫病杂志, 2021, 39(6): 842-847. DOI: 10.12140/j.issn.1000-7423.2021.06.018.XUE T, DU WQ. Progress in genotyping of pneumocystis jirovecii[J]. Chin J Parasitol Parasit Dis, 2021, 39(6): 842-847. DOI: 10.12140/j.issn.1000-7423.2021.06.018. [13] 孟静, 李光才, 肖建生, 等. 不同免疫状态下卡氏肺孢子菌肺炎临床特征的差异性分析[J]. 华中科技大学学报(医学版), 2021, 50(2): 225-229. DOI: 10.3870/j.issn.1672-0741.2021.02.016.MENG J, LI GC, XIAO JS, et al. Difference analysis of the clinical features of pneumocystis carinii pneumonia under different immune status[J]. Acta Med Univ Sci Technol Huazhong, 2021, 50(2): 225-229. DOI: 10.3870/j.issn.1672-0741.2021.02.016. [14] 王明明, 杨学敏. 肾移植术后患者肺孢子菌肺炎临床特征分析[J]. 临床肺科杂志, 2020, 25(9): 1355-1358. DOI: 10.3969/j.issn.1009-6663.2020.09.014.WANG MM, YANG XM. Clinical characteristics of pneumocystis pneumonia in patients after renal transplantation[J]. J Clin Pulm Med, 2020, 25(9): 1355-1358. DOI: 10.3969/j.issn.1009-6663.2020.09.014. [15] TASAKA S. Recent advances in the diagnosis and management of pneumocystis pneumonia[J]. Tuberc Respir Dis (Seoul), 2020, 83(2): 132-140. DOI: 10.4046/trd.2020.0015. [16] HAMMARSTRÖM H, GRANKVIST A, BROMAN I, et al. Serum-based diagnosis of pneumocystis pneumonia by detection of pneumocystis jirovecii DNA and 1, 3-β-D-glucan in HIV-infected patients: a retrospective case control study[J]. BMC Infect Dis, 2019, 19(1): 658. DOI: 10.1186/s12879-019-4289-4. [17] GUEGAN H, ROBERT-GANGNEUX F. Molecular diagnosis of pneumocystis pneumonia in immunocompromised patients[J]. Curr Opin Infect Dis, 2019, 32(4): 314-321. DOI: 10.1097/QCO.0000000000000559. [18] ZHAN Y, GAO X, LI S, et al. Development and evaluation of rapid and accurate CRISPR/Cas13-based RNA diagnostics for pneumocystis jirovecii pneumonia[J]. Front Cell Infect Microbiol, 2022, 12: 904485. DOI: 10.3389/fcimb.2022.904485. [19] WANG J, HAN Y, FENG J. Metagenomic next-generation sequencing for mixed pulmonary infection diagnosis[J]. BMC Pulm Med, 2019, 19(1): 252. DOI: 10.1186/s12890-019-1022-4. [20] LU X, ZHANG J, MA W, et al. Pneumocystis jirovecii pneumonia diagnosis via metagenomic next-generation sequencing[J]. Front Med (Lausanne), 2022, 9: 812005. DOI: 10.3389/fmed.2022.812005. [21] 冯玲, 熊佳丽, 易荣, 等. 宏基因组二代测序在肺部感染诊治的临床价值[J]. 临床肺科杂志, 2021, 26(12): 1834-1838. DOI: 10.3969/j.issn.1009-6663.2021.12.011.FENG L, XIONG JL, YI R, et al. Clinical value of metagenomic next-generation sequencing in diagnosis and treatment of pulmonary infection[J]. J Clin Pulm Med, 2021, 26(12): 1834-1838. DOI: 10.3969/j.issn.1009-6663.2021.12.011. [22] 沈轶, 潘雁, 尹成胜, 等. 二代测序诊断肺移植后耶氏肺孢子菌肺炎二例并文献复习[J]. 中国呼吸与危重监护杂志, 2021, 20(7): 479-486. DOI: 10.7507/1671-6205.202104007.SHEN Y, PAN Y, YIN CS, et al. Pneumocystis jirovecii pneumonia diagnosed by next-genetation sequencing after lung transplantation: case report and literature review[J]. Chin J Respir Crit Care Med, 2021, 20(7): 479-486. DOI: 10.7507/1671-6205.202104007. [23] 张彩霞, 刘新年, 杜川, 等. mNGS技术和血清G试验在判断耶氏肺孢子菌感染与定植中的价值及二者相关性研究[J]. 中国全科医学, 2023, 26(11): 1355-1360. DOI: 10.12114/j.issn.1007-9572.2022.0594.ZHANG CX, LIU XN, DU C, et al. mNGS and serum G test in distinguishing between pneumocystis jirovecii colonization and infection: value comparison and correlation analysis[J]. Chin Gen Pract, 2023, 26(11): 1355-1360. DOI: 10.12114/j.issn.1007-9572.2022.0594. [24] LIU L, YUAN M, SHI Y, et al. Clinical performance of BAL metagenomic next-generation sequence and serum (1, 3)-β-D-glucan for differential diagnosis of pneumocystis jirovecii pneumonia and pneumocystis jirovecii colonization[J]. Front Cell Infect Microbiol, 2021, 11: 784236. DOI: 10.3389/fcimb.2021.784236. [25] BATEMAN M, OLADELE R, KOLLS JK. Diagnosing pneumocystis jirovecii pneumonia: a review of current methods and novel approaches[J]. Med Mycol, 2020, 58(8): 1015-1028. DOI: 10.1093/mmy/myaa024. [26] LEE G, KOO TY, KIM HW, et al. Comparison of early and late pneumocystis jirovecii pneumonia in kidney transplant patients: the Korean Organ Transplantation Registry (KOTRY) study[J]. Sci Rep, 2022, 12(1): 10682. DOI: 10.1038/s41598-022-14580-5. [27] KUMAR D, GOURISHANKAR S, MUELLER T, et al. pneumocystis jirovecii pneumonia after rituximab therapy for antibody-mediated rejection in a renal transplant recipient[J]. Transpl Infect Dis, 2009, 11(2): 167-170. DOI: 10.1111/j.1399-3062.2008.00345.x. [28] PERRIER Q, PORTAIS A, TERREC F, et al. A case of pneumocystis jirovecii pneumonia under belatacept and everolimus: benefit-risk balance between renal allograft function and infection[J]. Case Rep Nephrol Dial, 2021, 11(1): 10-15. DOI: 10.1159/000510842. [29] AZAR MM, COHEN E, MA L, et al. Genetic and epidemiologic analyses of an outbreak of pneumocystis jirovecii pneumonia among kidney transplant recipients in the United States[J]. Clin Infect Dis, 2022, 74(4): 639-647. DOI: 10.1093/cid/ciab474. [30] KAMINSKI H, BELLIERE J, BURGUET L, et al. Identification of predictive markers and outcomes of late-onset pneumocystis jirovecii pneumonia in kidney transplant recipients[J]. Clin Infect Dis, 2021, 73(7): e1456-e1463. DOI: 10.1093/cid/ciaa1611. [31] ZOU J, QIU T, ZHOU J, et al. Clinical manifestations and outcomes of renal transplantation patients with pneumocystis jirovecii pneumonia and cytomegalovirus co-infection[J]. Front Med (Lausanne), 2022, 9: 860644. DOI: 10.3389/fmed.2022.860644. [32] LEE S, PARK Y, KIM SG, et al. The impact of cytomegalovirus infection on clinical severity and outcomes in kidney transplant recipients with pneumocystis jirovecii pneumonia[J]. Microbiol Immunol, 2020, 64(5): 356-365. DOI: 10.1111/1348-0421.12778. [33] DUAN J, GAO J, LIU Q, et al. Characteristics and prognostic factors of non-HIV immunocompromised patients with pneumocystis pneumonia diagnosed by metagenomics next-generation sequencing[J]. Front Med (Lausanne), 2022, 9: 812698. DOI: 10.3389/fmed.2022.812698. [34] MEYER AMJ, SIDLER D, HIRZEL C, et al. Distinct clinical and laboratory patterns of pneumocystis jirovecii pneumonia in renal transplant recipients[J]. J Fungi (Basel), 2021, 7(12): 1072. DOI: 10.3390/jof7121072. [35] LING J, ANDERSON T, WARREN S, et al. Hypercalcaemia preceding diagnosis of pneumocystis jirovecii pneumonia in renal transplant recipients[J]. Clin Kidney J, 2017, 10(6): 845-851. DOI: 10.1093/ckj/sfx044. [36] MARTIN SI, FISHMAN JA, AST Infectious Diseases Community of Practice. pneumocystis pneumonia in solid organ transplantation[J]. Am J Transplant, 2013, 13(Suppl 4): 272-279. DOI: 10.1111/ajt.12119. [37] 段艳, 徐媛, 杨长青, 等. 复方磺胺甲 [38] 姚芳, 路敏, 孔妍, 等. 耶氏肺孢子虫肺炎患者复方磺胺甲 [39] TU GW, JU MJ, XU M, et al. Combination of caspofungin and low-dose trimethoprim/sulfamethoxazole for the treatment of severe pneumocystis jirovecii pneumonia in renal transplant recipients[J]. Nephrology (Carlton), 2013, 18(11): 736-742. DOI: 10.1111/nep.12133.PMID:24571744. [40] JI J, WANG Q, HUANG T, et al. Efficacy of low-dose trimethoprim/sulfamethoxazole for the treatment of pneumocystis jirovecii pneumonia in deceased donor kidney recipients[J]. Infect Drug Resist, 2021, 14: 4913-4920. DOI: 10.2147/IDR.S339622. [41] GU ZY, LIU WJ, HUANG DL, et al. Preliminary study on the combination effect of clindamycin and low dose trimethoprim-sulfamethoxazole on severe pneumocystis pneumonia after renal transplantation[J]. Front Med (Lausanne), 2022, 9: 827850. DOI: 10.3389/fmed.2022.827850. -

 下载:
下载:

 点击查看大图
点击查看大图
图(3) / 表(2)
计量
- 文章访问数: 202
- HTML全文浏览量: 72
- PDF下载量: 69
- 被引次数: 0


