

Clinical technical operation specification for pathology of organ transplantation (2019 edition): heart transplantation
-
摘要: 为了进一步规范器官移植病理学临床技术操作,中华医学会器官移植学分会组织器官移植专家和移植病理学专家,从移植心脏心内膜心肌活组织检查的临床操作规范、移植心脏排斥反应的病理学诊断临床技术操作规范、移植心脏的心肌缺血损伤的病理学诊断临床技术操作规范、移植心脏血管病的病理学诊断临床技术操作规范、移植后淋巴组织增生性疾病的病理学诊断临床技术操作规范、移植心脏心内膜心肌活组织检查病理报告的基本内容规范、移植心脏心内膜心肌活组织检查病理学诊断的难点与局限性、移植心脏病理学相关的其它临床技术操作规范等方面,制定器官移植病理学临床技术操作规范(2019版)之移植心脏病理学临床技术操作规范。
-
关键词:
- 移植病理学 /
- 器官移植 /
- 心脏移植 /
- 心内膜心肌活组织检查 /
- 排斥反应 /
- 心肌缺血损伤 /
- 移植心脏血管病 /
- 移植后淋巴组织增生性疾病
-

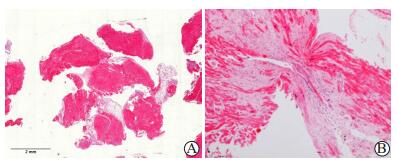
图 1 组织块充足的活检和前次活检部位的病理学特征
A图示EMB最大切面,组织块数量、大小、心肌组织比例均符合要求(标尺2.0 mm);B图示EMB活检组织内可见前次活检后在心内膜下形成的局灶性纤维疤痕组织,其中无单个核细胞浸润(HE,×100)
Figure 1. Pathological characteristics of biopsy with sufficient tissue mass and previous biopsy site

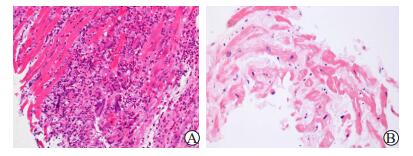
图 2 不同病理分级移植心脏急性细胞性排斥反应的病理学特征
A图为ACR 1R级,心肌间质局灶性少量单个核细胞浸润,但无明确心肌损伤(HE,×200);B图为ACR 1R级,心肌间质内单个局灶性的、较密集的单个核细胞浸润伴心肌细胞损伤(HE,×200);C图为ACR 2R级,心肌活检组织内两处局灶性的、密集的单个核细胞浸润,伴心肌细胞损伤并被炎性浸润替代,两处炎症灶接近融合(HE,×200);D图为ACR 3R级,心肌组织间质内弥漫性的、大量的单个核细胞浸润伴多灶心肌细胞损伤,心肌正常组织结构破坏(HE,×400)
Figure 2. Pathological characteristics of acute cellular rejection of cardiac allograft with different pathological grades

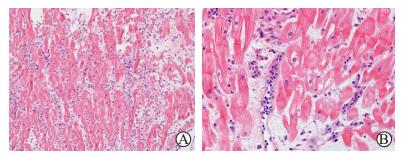
图 3 移植心脏抗体介导的排斥反应的组织病理学特征
A图示心肌间质水肿,毛细血管扩张,伴血管内细胞数量增多(HE,×200);B图示心肌间毛细血管内皮肿胀伴腔内巨噬细胞淋巴细胞聚集(活化的单个核细胞),呈组织病理学阳性(HE,×400)
Figure 3. Histopathological characteristics of antibody-mediated rejection in cardiac allograft

图 4 移植心脏抗体介导的排斥反应的免疫病理学特征(免疫组化,×200)
A图示多数心肌间毛细血管内皮可见C4d阳性的线样沉积,呈免疫病理学阳性;B图示较多心肌间毛细血管内可见CD68阳性巨噬细胞聚集,呈免疫病理学阳性
Figure 4. Immunopathological characteristics of antibody-mediated rejection in cardiac allograft

图 5 移植心脏Quilty病变的组织病理学特征(HE,×200)
A图示EMB活检组织内心内膜下部位局灶性、结节性单个核细胞浸润(↑);B图示心内膜淋巴细胞向深部扩展、浸润破坏浅层心肌;C图为B图邻近切面,可见ACR样改变
Figure 5. Histopathological characteristics of Quilty effect in cardiac allograft

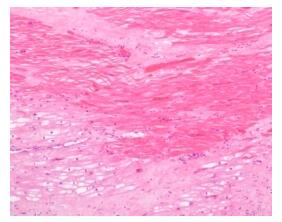
图 6 移植心脏后期心肌缺血损伤的病理学特征(HE,×200)
图示因慢性排斥反应所致的移植心脏血管病,引起心肌局灶凝固性坏死伴较广泛空泡变性
Figure 6. Pathological characteristics of late myocardial ischemia injury in cardiac allograft

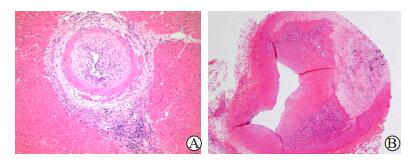
图 7 移植心脏血管病与冠状动脉粥样硬化的病理学特征
A图示CAV壁内小动脉内膜同心性纤维肌性增生伴内膜炎和动脉周围炎(HE,×100);B图示移植心脏心表冠状动脉偏心性粥样硬化斑块内脂质沉积、纤维化、钙化(HE,×20)
Figure 7. Pathological characteristics of cardiac allograft vasculopathy and coronary artery atherosclerosis

图 8 心脏移植术前选择性EMB的病理学发现(HE,×400)
A图示巨细胞性心肌炎,可见心肌局灶坏死,大量单核淋巴细胞和较多嗜酸性粒细胞浸润,多核巨细胞易见,但无明显的肉芽肿结节形成;B图示心肌淀粉样变性,心肌细胞间隙加宽,可见粉染、均质的淀粉样物质沉积
Figure 8. Pathological findings of selective EMB in the patients before cardiac transplantation
表 1 移植心脏急性细胞性排斥反应的病理分级(ISHLT 2004年)[7]
Table 1. Pathological classification of acute cellular rejection in cardiac allograft (ISHLT 2004)
级别 组织病理学改变 0R 无排斥反应 1R,轻度 间质或(和)血管周的炎性浸润,伴最多一灶心肌损伤 2R,中度 两灶或多灶炎性浸润伴相关的心肌损伤 3R,重度 弥漫的炎性浸润伴多灶心肌损伤±水肿±出血±血管炎 R为ISHLT 2004年修订的级别,以区别于ISHLT 1990年的分级  下载: 导出CSV
下载: 导出CSV
表 2 移植心脏抗体介导性排斥反应的组织病理学诊断标准(ISHLT 2013年)[8]
Table 2. Histopathological diagnostic criteria of antibody-mediated rejection in cardiac allograft (ISHLT 2013)
形态学标准 病理所见 血管内活化的单个核细胞 心肌间毛细血管和小静脉内巨噬细胞聚集、扩张和充填血管腔 内皮细胞胞核增大、胞浆肿胀,血管腔狭窄或梗阻 重度AMR 心肌间质水肿、出血,心肌细胞坏死,毛细血管碎裂,混合的炎性细胞浸润,内皮细胞核固缩和(或)核碎裂
下载: 导出CSV
表 3 移植心脏抗体介导性排斥反应的病理学诊断分级方案(ISHLT 2013年)[6]
Table 3. Pathological grading diagnosis of antibody-mediated rejection in cardiac allograft
分级 定义 病理基质 pAMR 0 病理学的AMR阴性 组织学和免疫病理学实验双阴性 pAMR 1(H+) 单一组织病理学的AMR 组织学阳性,而免疫病理学阴性 pAMR 1(I+) 单一免疫病理学的AMR 组织学阴性,而免疫病理学阳性[CD68阳性和(或)C4d阳性] pAMR 2 病理学的AMR 组织学和免疫病理学双阳性 pAMR 3 重度病理学的AMR 间质出血,毛细血管破裂,混合的炎性细胞浸润,内皮细胞核固缩和(或)核碎裂,明显的水肿并有免疫病理学阳性。与重度的血流动力学异常和不良预后相关
下载: 导出CSV
表 4 移植心脏抗体介导性排斥反应的临床分期[10]
Table 4. Clinical stages of antibody-mediated rejection in cardiac allograft
顺序 AMR分期 主要特征 1 亚临床期 DSA阳性,无移植心功能损伤或衰竭的病理学证据 2 临床前期 有移植心功能损伤的病理学证据,但无心功能衰竭,无临床症状 3 急性临床期 有移植心功能损伤的病理学证据,有心功能衰竭,有或无临床症状 4 慢性期 移植心脏血管病,或慢性移植物功能衰竭,或限制性心脏生理学改变 限制性心脏生理学改变指心脏射血分数保留的心功能受损状态
下载: 导出CSV
表 5 移植心脏血管病与冠状动脉粥样硬化的血管病理学特征比较
Table 5. Comparison of vascular pathological features between cardiac allograft vasculopathy and coronary artery atherosclerosis
病理学特征 移植心脏血管病 冠状动脉粥样硬化 受累血管 所有血管类型,主要累及壁内血管 近端冠状动脉 斑块类型 弥漫,同心性 局灶,偏心性 血管炎症 有 罕见 内弹力板 完整 破坏 钙盐沉积 无 有
下载: 导出CSV
-
[1] 黄洁, 杨跃进, 尹栋, 等.心内膜心肌活检439例次的安全性分析[J].中华心血管病杂志, 2010, 38(1):43-46. DOI: 10.3760/cma.j.issn.0253-3758.2010.01.013.HUANG J, YANG YJ, YIN D, et al. Safety analyses from 439 patients underwent endomyocardial biopsy[J]. Chin J Cardiol, 2010, 38(1):43-46. DOI: 10.3760/cma.j.issn.0253-3758.2010.01.013. [2] FIORELLI AI, BENVENUTI L, AIELO V, et al. Comparative analysis of the complications of 5347 endomyocardial biopsies applied to patients after heart transplantation and with cardiomyopathies: a single-center study[J]. Transplant Proc, 2012, 44(8):2473-2478. DOI: 10.1016/j.transproceed.2012.07.023. [3] LAMPERT BC, TEUTEBERG JJ, SHULLO MA, et al. Cost-effectiveness of routine surveillance endomyocardial biopsy after 12 months post-heart transplantation[J]. Circ Heart Fail, 2014, 7(5):807-813. DOI: 10.1161/CIRCHEARTFAILURE.114.001199. [4] LUND LH, EDWARDS LB, KUCHERYAVAYA AY, et al. The Registry of the International Society for Heart and Lung Transplantation: thirty-second official adult heart transplantation report--2015; focus theme: early graft failure[J]. J Heart Lung Transplant, 2015, 34(10):1244-1254. DOI: 10.1016/j.healun.2015.08.003. [5] LI L, DUAN XJ, WANG HY, et al. Acute cellular rejection and antibody-mediated rejection in endomyocardial biopsy after heart transplantation: a retrospective study from a single medical center[J]. Int J Clin Exp Pathol, 2017, 10(4):4772-4779. [6] BERRY GJ, BURKE MM, ANDERSEN C, et al. The 2013 International Society for Heart and Lung Transplantation working formulation for the standardization of nomenclature in the pathologic diagnosis of antibody-mediated rejection in heart transplantation[J]. J Heart Lung Transplant, 2013, 32(12):1147-1162. DOI: 10.1016/j.healun.2013.08.011. [7] STEWART S, WINTERS GL, FISHBEIN MC, et al. Revision of the 1990 working formulation for the standardization of nomenclature in the diagnosis of heart rejection[J]. J Heart Lung Transplant, 2005, 24(11):1710-1720. doi: 10.1016/j.healun.2005.03.019 [8] LEONE O, VEINOT JP, ANGELINI A, et al.2011 consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology[J]. Cardiovasc Pathol, 2012, 21(4):245-274. DOI: 10.1016/j.carpath.2011.10.001. [9] HAAS M, SIS B, RACUSEN LC, et al. Banff 2013 meeting report: inclusion of C4d-negative antibody-mediated rejection and antibody-associated arterial lesions[J]. Am J Transplant, 2014, 14(2):272-283. DOI: 10.1111/ajt.12590. [10] COLVIN MM, COOK JL, CHANG P, et al.Antibody-mediated rejection in cardiac transplantation: emerging knowledge in diagnosis and management: a scientific statement from the American Heart Association[J]. Circulation, 2015, 131(18):1608-1639. DOI: 10.1161/CIR.0000000000000093. [11] MILLER DV, KFOURY AG. "Mixed" rejection in heart transplantation[M]// LEONE O, ANGELINI A, BRUNEVAL P, et al. The pathology of cardiac transplantation: clinical and pathological perspective. Switzerland: Springer International Publishing, 2016: 243-250. [12] TAN CD, BALDWIN WM 3RD, RODRIGUEZ ER. Update on cardiac transplantation pathology[J]. Arch Pathol Lab Med, 2007, 131(8):1169-1191. [13] JOSHI A, MASEK MA, BROWN BW JR, et al. "Quilty" revisited: a 10-year perspective[J]. Hum Pathol, 1995, 26(5):547-557. DOI: 10.1016/0046-8177(95)90252-X. [14] FYFE B, LOH E, WINTERS GL, et al. Heart transplantation-associated perioperative ischemic myocardial injury. morphological features and clinical significance[J]. Circulation, 1996, 93(6):1133-1140. DOI: 10.1161/01.CIR.93.6.1133. [15] LU WH, PALATNIK K, FISHBEIN GA, et al.Diverse morphologic manifestations of cardiac allograft vasculopathy: a pathologic study of 64 allograft hearts[J]. J Heart Lung Transplant, 2011, 30(9):1044-1050. DOI: 10.1016/j.healun.2011.04.008. [16] MEHRA MR, CRESPO-LEIRO MG, DIPCHAND A, et al. International Society for Heart and Lung Transplantation working formulation of a standardized nomenclature for cardiac allograft vasculopathy-2010[J]. J Heart Lung Transplant, 2010, 29(7):717-727. DOI: 10.1016/j.healun.2010.05.017. [17] SABATTINI E, BACCI F, SAGRAMOSO C, et al. WHO classification of tumours of haematopoietic and lymphoid tissues in 2008: an overview[J]. Pathologica, 2010, 102(3):83-87. [18] CRESPO-LEIRO MG, ZUCKERMANN A, BARA C, et al.Concordance among pathologists in the second Cardiac Allograft Rejection Gene Expression Observational Study (CARGO Ⅱ)[J]. Transplantation, 2012, 94(11):1172-1177. DOI: 10.1097/TP.0b013e31826e19e2. [19] ANGELINI A, ANDERSEN CB, BARTOLONI G, et al. A web-based pilot study of inter-pathologist reproducibility using the ISHLT 2004 working formulation for biopsy diagnosis of cardiac allograft rejection: the European experience[J]. J Heart Lung Transplant, 2011, 30(11):1214-1220. DOI: 10.1016/j.healun.2011.05.011. [20] COOPER LT, BAUGHMAN KL, FELDMAN AM, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology[J]. Circulation, 2007, 116(19):2216-2233. DOI: 10.1161/circulationaha.107.186093. [21] STONE JR, BASSO C, BAANDRUP UT, et al. Recommendations for processing cardiovascular surgical pathology specimens: a consensus statement from the Standards and Definitions Committee of the Society for Cardiovascular Pathology and the Association for European Cardiovascular Pathology[J]. Cardiovasc Pathol, 2012, 21(1):2-16. DOI: 10.1016/j.carpath.2011.01.001. [22] BASSO C, BURKE M, FORNES P, et al. Guidelines for autopsy investigation of sudden cardiac death[J]. Virchows Arch, 2008, 452(1):11-18. DOI: 10.1007/s00428-007-0505-5. -

 下载:
下载:




 点击查看大图
点击查看大图
计量
- 文章访问数: 338
- HTML全文浏览量: 133
- PDF下载量: 97
- 被引次数: 0


